

Summary
Treatment of idiopathic pulmonary arterial hypertension (PAH) with the β-blocker bisoprolol resulted in decreased heart rate, increased right ventricular ejection fraction (RVEF), and improved quality of life. This article presents data from the Beta-Blocker Therapy in Idiopathic Pulmonary Arterial Hypertension trial [NCT01246037; Van Campen JSJA et al. Am J Respir Crit Care 2014].
- Thromboembolic Disease
- Pulmonary Clinical Trials
- Hypertensive Disease
- Pulmonary & Critical Care
- Thromboembolic Disease
- Pulmonary Clinical Trials
- Hypertensive Disease
Treatment of idiopathic pulmonary arterial hypertension (PAH) with the β-blocker bisoprolol resulted in decreased heart rate, increased right ventricular ejection fraction (RVEF), and improved quality of life (QoL). J.S.J.A. Van Campen, MD, VU Medical Center, Amsterdam, The Netherlands, presented data from the Beta-Blocker Therapy in Idiopathic Pulmonary Arterial Hypertension trial [NCT01246037; Van Campen JSJA et al. Am J Respir Crit Care 2014].
The sympathetic nervous system is excessively active in PAH; however, blockade by β-blockers was thought to be contraindicated because of the acute negative inotropic and chronotropic effects. Despite similar thinking, blockade of β-adrenergic receptors in patients with left heart failure has been shown to reduce left ventricular remodeling and mortality by about 30% [Dickstein K et al. Eur Heart J 2008]. In addition, data from recent preclinical animal studies suggest that low-dose β-blocker therapy may be beneficial in PAH [De Man FS et al. Circ Heart Fail 2012]. The purpose of this study was to determine if bisoprolol is safe and effective in patients with PAH.
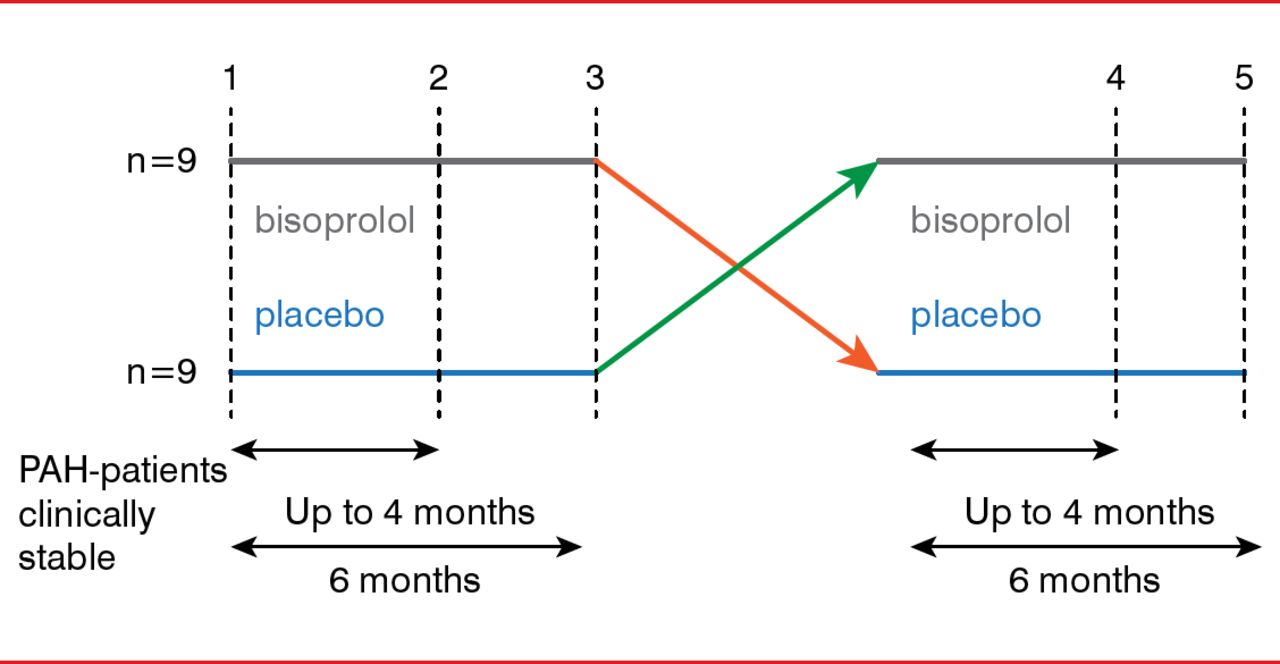
In this double-blind, crossover, Phase 1 and 2 trial, 18 patients with optimally treated, stable idiopathic PAH received an escalating dose of up to 10 mg of bisoprolol or placebo for up to 6 months, then crossed over to the opposite treatment for up to an additional 6 months (Figure 1). Patients were assessed every 2 weeks by physical examination with blood pressure and heart rate measurements. Every month, patients underwent electrocardiography, 6-minute walking distance (6MWD) tests, and the Minnesota Living With Heart Failure Questionnaire assessing QoL. In addition, at baseline, crossover, and end of the study, patients were evaluated by magnetic resonance imaging (MRI), echocardiography, heart rate variability measurements, cardiopulmonary exercise testing, and positron emission tomography.

Trial Design of the Beta-Blocker Therapy in Idiopathic PAH Trial
PAH=pulmonary arterial hypertension.
Reproduced with permission from JSJA Van Campen, MD.
The primary end point of the study was RVEF, as measured by cardiac MRI. The secondary end points included assessments of sympathetic overdrive, maladaptive remodeling of the right ventricular wall, perfusion, mechanical efficiency, and exercise capacity.
Patients who received bisoprolol (mean dose, 4.4 ± 3.2 mg) demonstrated an improvement in RVEF by 3%, which was not statistically significant. However, bisoprolol treatment resulted in a significant decrease in heart rate (p=0.0001), with most patients (15 of 18) experiencing reductions of 10 beats/min. Significant decreases were also seen in cardiac output (p=0.02) and cardiac output, as measured by the 6-minute walk test (p<0.02). There were no significant differences in maximal oxygen consumption or QoL.
Of 18 patients, 5 experienced serious adverse effects; however, 4 events were determined to not be associated with the study drug. One patient experienced fluid retention at the beginning of bisoprolol treatment that required intravenous diuretics. Two patients did not tolerate bisoprolol, secondary to hypotension, bradycardia, or fatigue. Syncope was not reported during the study.
In conclusion, Prof. van Campen stated that data from this trial indicated that treatment of PAH with a β-blocker is safe and well tolerated. In addition, β-blocker treatment can reduce heart rate and improve RVEF and QoL, without significantly affecting exercise capacity.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.