

Summary
This article discusses the critical need to control blood pressure (BP) for patients with chronic kidney disease, issues in diagnosis and management, and specific issues in patients with end-stage renal disease.
- Hypertension & Kidney Disease
- Hypertensive Disease
- Renal Disease
- Cardiology & Cardiovascular Medicine
- Hypertension & Kidney Disease
- Hypertensive Disease
- Renal Disease
In a session at the Joint Meeting of the European Society of Hypertension and International Society of Hypertension on hypertension in chronic kidney disease (CKD), a panel of experts discussed the critical need to control blood pressure (BP) for patients with CKD, issues in diagnosis and management, and specific issues in patients with end-stage renal disease (ESRD).
CHANGING EPIDEMIOLOGY OF CKD: INCREASING NUMBER OF PEOPLE WITH UNCONTROLLED BP AT RISK OF DEVELOPING CKD AND ESRD
Roland E. Schmieder, MD, Professor of Internal Medicine, Nephrology, and Hypertension, University Hospital Erlangen, Erlangen, Germany, opened the session with an overview of the changing epidemiology of CKD in the general population. He highlighted that hypertension and diabetes are the major contributors to the increasing prevalence of CKD, causing up to 60% of cases of CKD in 2014. Hypertension is the primary contributor to progressive disease, he said, indicating that better BP control is critical to slowing down the increasing incidence of ESRD. Data from the Framingham Offspring study showed that the lifetime risk of developing ESRD in the general population was 9.4% [Drev N et al. Am J Kidney Dis 2003] and that the incidence increased with advancing age, diabetes, hypertension, smoking, obesity, and a lower baseline glomerular filtration rate (GFR).
To reduce the incidence of ESRD and to better manage patients with CKD, patients who are at high risk of developing renal and cardiovascular disease need to be identified. Two tools—estimated GFR (eGFR) and urine albumin-to-creatinine ratio (UACR)—were reviewed and described as having strong predictive power to identify patients with CKD at high risk. Data show that eGFR and UACR were multiplicatively associated with risk of all-cause and cardiovascular mortality, with eGFR <60 mL/minute/1.73 m2 and UACR >1.1 mg/mmol (10 mg/g) as independent predictors of mortality risk in the general population [Chronic Kidney Disease Prognosis Consortium. Lancet 2010].
Dr. Schmieder emphasized that estimation of GFR is essential for both the staging and the management of CKD (Table 1) [National Kidney Foundation. Am J Kidney Dis 2002].
Importance of GFR for Appropriate Staging and Management of Chronic Kidney Disease
Overall, he stated that better BP control is essential, and he highlighted that despite medical treatment, many patients have persistent uncontrolled BP [Peralta CA et al. Hypertens 2005; Hajjar I, Kotchen TA. JAMA 2003]. What is really needed, he concluded, are population-based strategies for prevention.
BP TARGETS IN PATIENTS WITH CKD
Gérard London, MD, Centre Hospitalier Manhès, Fleury-Mérogis Cedex, France, spoke on appropriate BP targets in patients with CKD based on the clinical practice guidelines developed by the Kidney Disease Improving Global Outcomes (KDIGO) [KDIGO. Kidney International Supplements 2012] He first described the process of generating and grading the recommendations as shown in Table 2.
Final Grading of the KDIGO Recommendations
Given the lack of high-quality evidence for most of the issues discussed in the guidelines, he emphasized that most of the recommendations provided are not based on the highest quality of evidence and that many of the guidelines offered only rise to the level of suggestion. Table 3 summarizes the recommendations based on the best evidence for the management of BP in patients with CKD.
Recommendations Based on the Best Evidence for Blood Pressure Management in Chronic Kidney Disease
DEGREE OF RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM BLOCKAGE IN HYPERTENSIVE PATIENTS WITH CKD
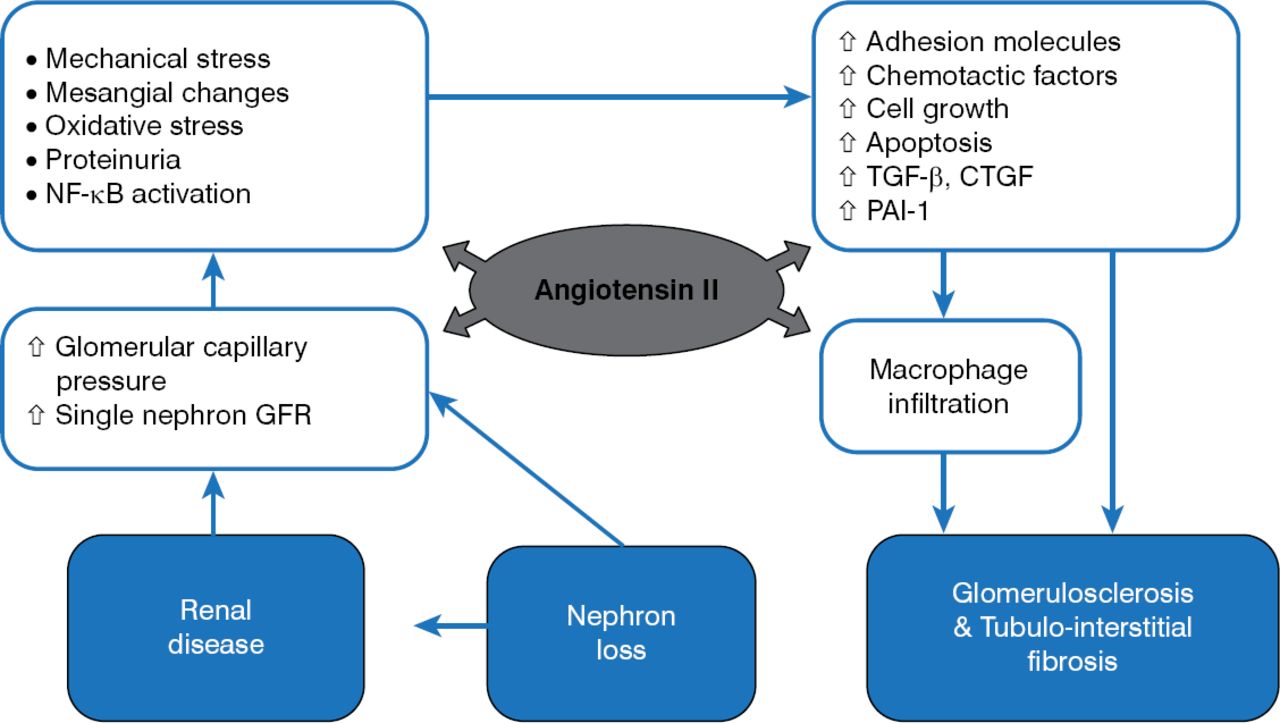
Pantelis A. Sarafidis, MD, Senior Lecturer and Honorary Consultant in Nephrology, Department of Nephrology, Hippkoration Hospital, Aristotle University, Thessaloniki, Greece, spoke on the degree of renin-angiotensin-aldosterone system (RAAS) blockade in hypertensive patients with CKD. Figure 1 illustrates the role of the RAAS on renal disease.

Angiotensin II and Kidney Injury
CTGF=connective tissue growth factor; GFR=glomerular filtration rate; PAI-1=plasminogen activator inhibitor-1; TGF-β=transforming growth factor-beta.
Reproduced with permission from PA Sarafidis, MD.
Dr. Sarafidis then described clinical data on the effect of RAAS inhibition on renal protection, highlighting that the benefit of RAAS inhibition is mainly in patients with proteinuric nephropathies or those with diabetes and microalbuminuria (Table 4) [Sarafidis P et al. Am J Kidney Dis 2007].
Major Randomized Clinical Trials on Renoprotective Effect of RAAS Inhibition
Although data show that renin-angiotensin system (RAS) blockers reduce progression of typical diabetic neuropathy from normo- to microalbuminuria and from micro- to macroalbuminuria, he stated that no specific agents are indicated in patients with diabetes, normoalbuminuria, and other causes of reduced eGFR (particularly in elderly patients). He also noted that elderly people are underrepresented in these clinical trials, and he emphasized the need to consider this. Specifically, RAS blockers and diuretics may increase the risk of prerenal acute renal failure in elderly persons—including other predisposed patients, such as those with renal arterial lesions or heart failure or those using radiocontrasts or nonsteroidal anti-inflammatory drugs—and that may translate into progression of CKD. For patients without diabetes and nonproteinuric CKD, he said that RAS inhibition and use of diuretics should be individualized, with close follow-up of renal function.
DIAGNOSIS AND MANAGEMENT OF HYPERTENSION IN ESRD PATIENTS
Carmine Zoccali, MD, Riuniti Hospital, Reggio Calabria, Italy, spoke on the diagnosis and management of hypertension in ESRD patients and the complex relationship between BP and outcomes in this population. Given the dips in BP in this population because of the differences in pre- and postdialysis BP, he clarified that hypertension in these patients mainly depends on volume expansion and that correcting fluid overload by long dialysis sessions in these patients reduces BP.
He indicated that because of the pre- and postdialysis fluctuations in BP based on fluid status, the use of the gold standard 24-hour BP monitoring is not reliable in this population. Instead, evidence from a joint position statement by the American Society of Hypertension and American Society of Nephrology supports estimating a first-time BP at 44 hours between 2 dialysis sessions with a new threshold for defining hypertension as 135/88 mm Hg (Agarwal R et al. J Am Soc Nephrol 2014). If only home monitoring is available, the guidelines recommend 48-hour monitoring, with hypertension defined as >140/90 mm Hg. He said that home monitoring is a good surrogate and is associated with better ambulatory BP monitoring than capturing pre- and posthemodialysis BP; furthermore, it tracks changes in BP evoked by reduction in body fluids, and it is more reproducible than pre- and posthemodialysis BP.
Among the interventions that he described to manage BP in this population was the use of ultrafiltration (UF) intensification, with evidence showing that UF intensification with constant dialysis duration reduces BP [Agarwal R et al. Hypertension 2009]. However, other data suggesting that UF intensification may increase adverse events in these patients [Curatola G et al. J Nephrol 2011] indicate the need for more thorough assessment via adequately powered studies to assess safety.
Reducing BP lowers cardiovascular risk in these patients, he said, but there is no evidence of pleiotropism by RAS blockade in these patients. Overall, he said that beta-blockade confers superior cardioprotection compared to angiotensin-converting-enzyme inhibition in these patients.
SESSION SUMMARY
In sum, the increasing prevalence of CKD and ESRD relates to the increasing prevalence of risk factors, such as hypertension and diabetes, and suboptimal risk factor control. RAAS blockade improves renal outcomes in patients with proteinuric nephropathies or those with diabetes and microalbuminuria. In those who have progressed to ESRD, BP typically reflects volume status. As such, a standardized approach to measurement and management of BP must take into account the time in relation to volume removal via dialysis or UF.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
- Article
- Summary
- CHANGING EPIDEMIOLOGY OF CKD: INCREASING NUMBER OF PEOPLE WITH UNCONTROLLED BP AT RISK OF DEVELOPING CKD AND ESRD
- BP TARGETS IN PATIENTS WITH CKD
- DEGREE OF RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM BLOCKAGE IN HYPERTENSIVE PATIENTS WITH CKD
- DIAGNOSIS AND MANAGEMENT OF HYPERTENSION IN ESRD PATIENTS
- SESSION SUMMARY
- Figures & Data
- Info & Metrics
- eLetters
Cited By...
- No citing articles found.