

Summary
This article reviews the background and design for the Reducing Atrial Pacing Rate to Reduce Atrial Fibrillation in Patients With Sick Sinus Syndrome study [DANPACE II; NCT02034526].
- Cardiology Clinical Trials
- Arrhythmias
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Arrhythmias
Jens Cosedis Nielsen, MD, Aarhus University Hospital, Skejby, Denmark, reviewed the background and design for the Reducing Atrial Pacing Rate to Reduce Atrial Fibrillation in Patients With Sick Sinus Syndrome study [DANPACE II; NCT02034526].
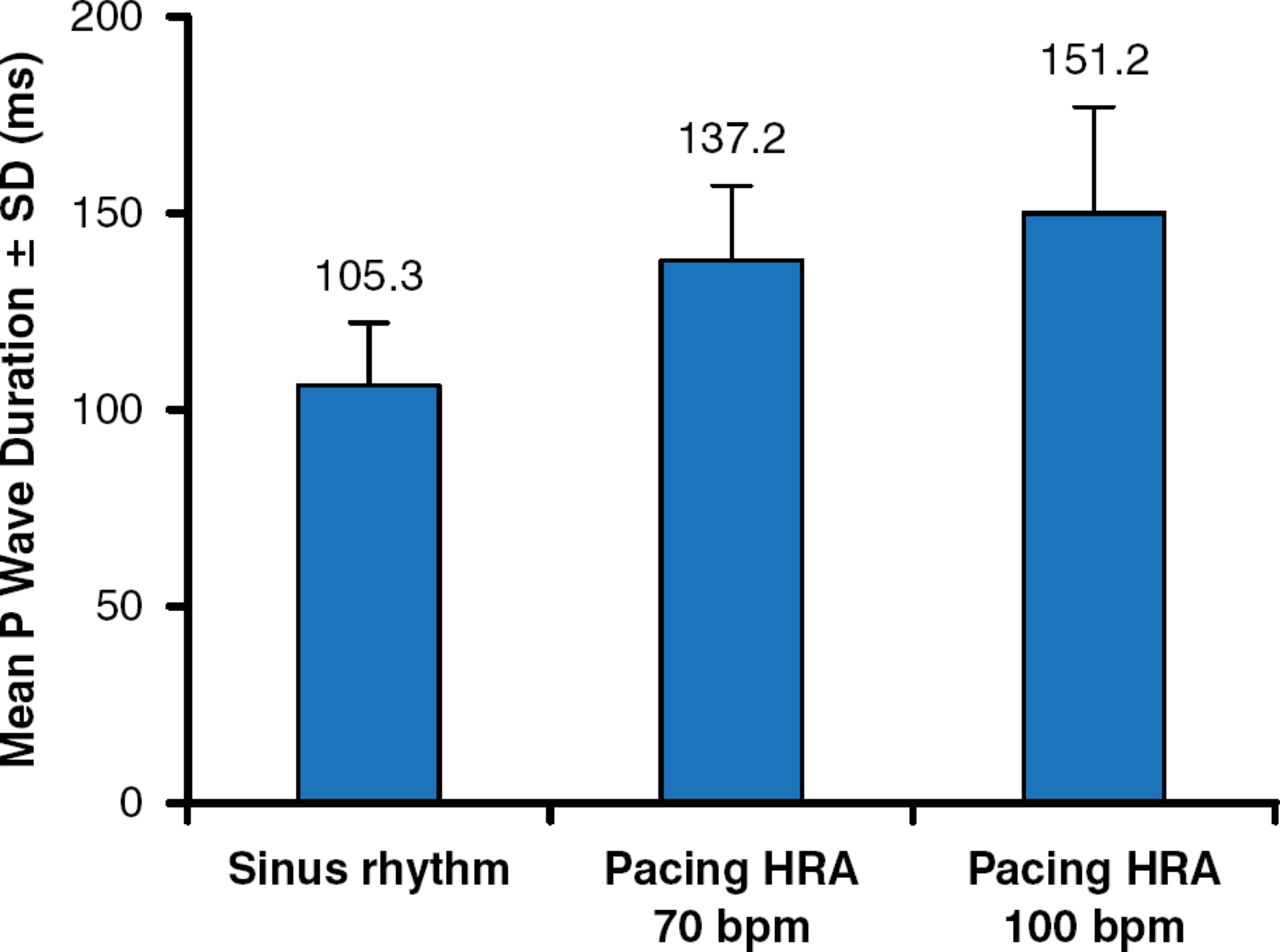
Atrial (A)-pacing may lead to prolonged and abnormal atrial activation and prolonged atrioventricular (AV) conduction, which in turn may increase ventricular pacing and thus may lead to atrial fibrillation (AF). A-pacing has been shown to cause P-wave prolongation, to induce P-wave axis changes, and to increase P-wave duration (Figure 1) [Kristensen L et al. Pacing Clin Electrophysiol 2004].

Effect of Atrial Pacing on P-Wave Duration
HRA=pacing at the high-rate atrium.
Reproduced with permission from John Wiley from Kristensen L, Nielsen JC, Mortensen PT, et al. Sinus and paced P wave duration and dispersion as predictors of atrial fibrillation after pacemaker implantation in patients with isolated sick sinus syndrome. Pacing Clin Electrophysiol 2004;27:606–614.
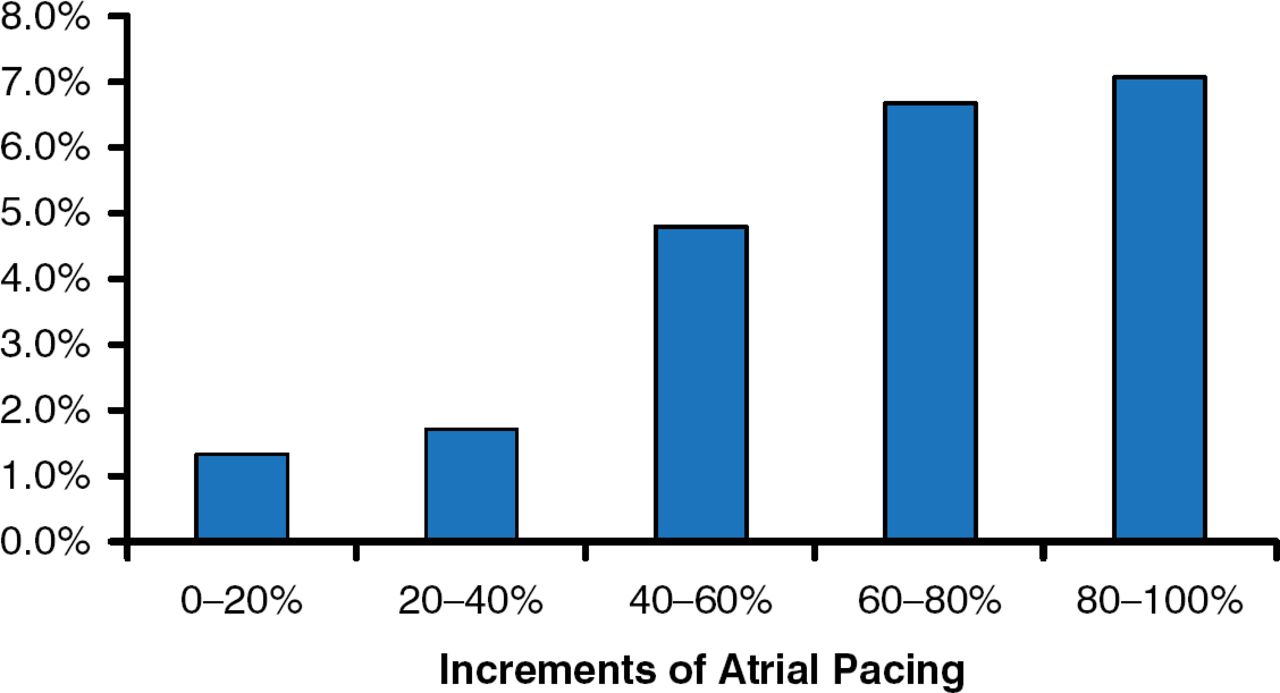
A meta-analysis has shown that the risk for AF is increased with A-pacing (Figure 2) and that rate-adaptive pacing causes more A-pacing [Elkayam LU et al. Pacing Clin Electrophysiol 2011]. The Advanced Elements of Pacing Randomized Controlled Trial [ADEPT] showed that there was no beneficial effect of rate-adaptive pacing on functional status or quality of life of patients with bradycardia indications for dual-chamber pacing [Lamas GA et al. Heart Rhythm 2007]. The Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial [ASSERT] showed that continuous atrial overdrive pacing did not prevent new-onset AF and was poorly tolerated [Hohnloser SH et al. Heart Rhythm 2012]. ASSERT also showed that AF >6 minutes in duration was associated with more atrial tachycardia and more thromboembolic events [Kaufman ES et al. Heart Rhythm 2012].

Atrial Pacing Increases Risk for Atrial Fibrillation
Reproduced with permission from John Wiley from Elkayam LU, Koehler JL, Sheldon TJ, et al. The influence of atrial and ventricular pacing on the incidence of atrial fibrillation: a meta-analysis. Pacing Clin Electrophysiol 2011;34:1593–1599.
However, it is unknown whether reducing A-pacing can reduce AF. The randomized, controlled DANPACE II trial will test in 900 patients whether dual-chamber pacing at 40 beats/min (DDD-40) reduces the incidence of AF ≥6 minutes compared with dual-chamber, adaptive-rate pacing at 60 beats/min (DDDR-60) in patients with sick sinus syndrome (SSS). Central remote monitoring will be conducted during the 2-year trial; all messages requiring clinical action will be sent to the local hospital of the patient.
The primary endpoint is the time to the first episode of pacemaker (PM)–detected AF >6 minutes. Secondary end points are the time to the first episode of PM-detected AF >6 hours and to >24 hours, number of AF episodes, percentage of time in AF, time to persistent AF, hospital admission because of AF, time to cardioversion for AF, time to PM reprogramming, time to event (stroke, transient cognitive impairment, or peripheral thromboembolism), time to death, quality of life, and 6-minute walk distance.
The inclusion criteria are patients aged ≥18 years with SSS and an indication for their first DDD PM (symptomatic sinus pause >2 seconds or sinus bradycardia with or without paroxysmal AF).
The exclusion criteria are permanent or persistent (>7 days) AF before PM implantation, persistent sinus bradycardia or symptomatic chronotropic incompetence (SCI) requiring DDD pacing at >40 beats/min, life expectancy < 1 year, grade II or III persistent AV block, indication for an implantable cardioverter-defibrillator or cardiac resynchronization therapy, pregnancy, or participation in another intervention study.
Patients with suspected SCI in the DDD-40 group will be crossed over to the DDDR-60 group after exercise testing and 24-hour Holter monitoring. After 1 month, they will be reevaluated, and patients whose symptoms are reduced will remain on DDDR-60.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.