

Summary
Primary Hyperparathyroidism (PHPT) is a common disorder, and surgery is a curative option for patients whose PHPT is symptomatic, unless there is a contraindication. The Guidelines for the Management of Asymptomatic PHPT are reviewed in this article.
- thyroid disorders
- diabetes & endocrinology guidelines
The Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism (PHPT) [Bilezikian JP et al. J Clin Endocrinol Metab 2014] were reviewed by John P. Bilezikian, MD, Columbia University College of Physicians and Surgeons, New York, New York, USA. PHPT is a common disorder, and surgery is a curative option for patients whose PHPT is symptomatic, unless there is a contraindication. For patients with asymptomatic PHPT, these evidence-based guidelines are intended to provide guidance to determine whether a surgical or medical approach should be used for management.
The development of the 2014 Guidelines was the objective of the 4th International Workshop on the Management of Asymptomatic PHPT, which was held in Florence, Italy, in September 2013. Four working groups focused on diagnosis, presentation, surgical management, and medical management, and a document on each of these areas will be published. A complete review of the peer-reviewed literature since 2008 served as the foundation for the evidence-based recommendations in the revised 2014 Guidelines.
DIAGNOSIS AND ASSESSMENT OF ASYMPTOMATIC PHPT
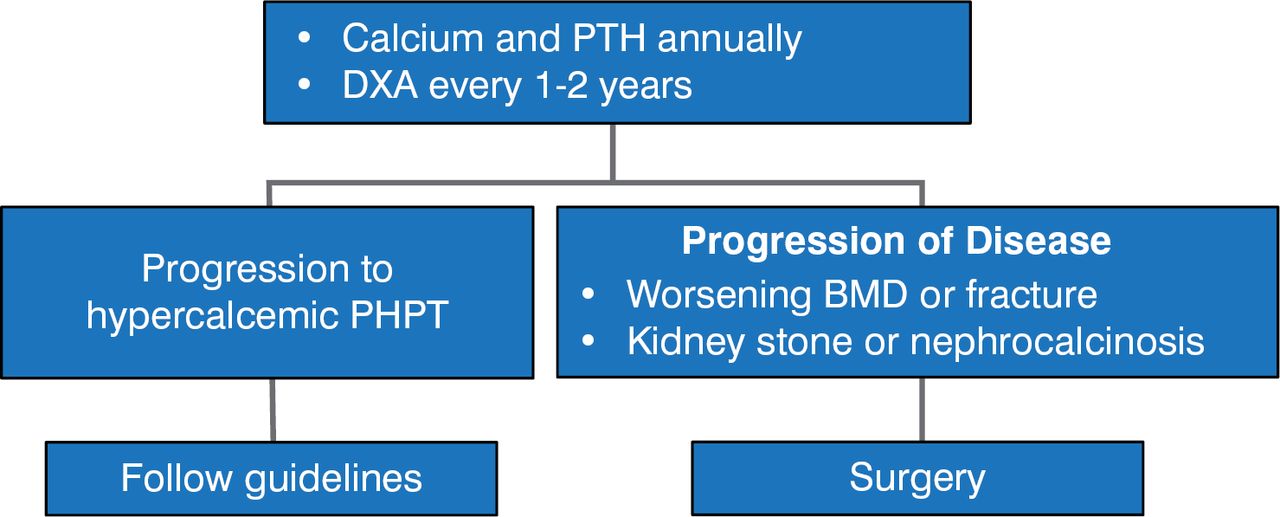
Normocalcemic PHPT is now recognized as a phenotype of PHPT, and its management approach is shown in Figure 1 [Bilezikian JP et al. J Clin Endocrinol Metab 2014]. In this phenotype, the initial presentation may be only elevated parathyroid hormone (PTH) levels.

Management of Asymptomatic Normocalcemic PHPT
BMD=bone mineral density; DXA=dual-energy X-ray absorptiometry; PHPT=primary hyperparathyroidism; PTH=parathyroid hormone.
Reproduced with permission from JD Bilezikian, MD.
A new hypothesis in the 2014 Guidelines states that PHPT is characterized by compromised cortical and trabecular compartments and an increased risk of fracture, even in asymptomatic PHPT. A skeletal assessment of PHPT is recommended; this includes dual-energy X-ray absorptiometry (DXA), and either vertebral fracture assessment (VFA), trabecular bone score (TBS), or vertebral X-rays. Recent studies showed that the majority of patients with asymptomatic PHPT had abnormal trabecular structure as measured by TBS [Silva BC et al. J Clin Endocrinol Metab 2013; Romagnoli E et al. Bone 2013]. Vertebral fractures are increased in PHPT, as shown by clinical studies [Vignali E et al. J Clin Endocrinol Metab 2009; Mosekilde L. Clin Endocrinol (Oxf) 2008], as are microstructural deficits [Hansen S et al. J Bone Miner Res 2012; Stein EM et al. J Bone Miner Res 2013].
Renal assessment of PHPT is recommended in the 2014 Guidelines to include 24 h urine analysis for calcium and other stone risk factors, and abdominal imaging. In patients with PHPT and an estimated glomerular filtration rate (eGFR) < 60 cc/min, there was evidence of more skeletal involvement, including altered bone remodeling [Walker MD et al. J Clin Endocrinol Metab 2012]. Kidney stones are the most common complication of PHPT and can be detected by noninvasive imaging.
The current data for the effect of PHPT on the neurocognitive and cardiovascular systems are insufficient to make recommendations for its surgical management, according to the 2014 Guidelines. It is known that the clinical manifestations of PHPT may be more severe in the presence of vitamin D deficiency; thus, the 2014 Guidelines recommend 25-OH vitamin D levels > 20 ng/mL, whereas calcium intake should follow the national guidelines, stated Dr. Bilezikian.
SURGICAL MANAGEMENT OF PHPT
Preoperative localization of the parathyroid, using computed tomography, ultrasound, or sestamibi scintigraphy, is mandatory before surgery. Surgical approaches are full exploration or a minimally invasive parathyroidectomy with intraoperative assessment of PTH levels, according to the 2014 Guidelines.
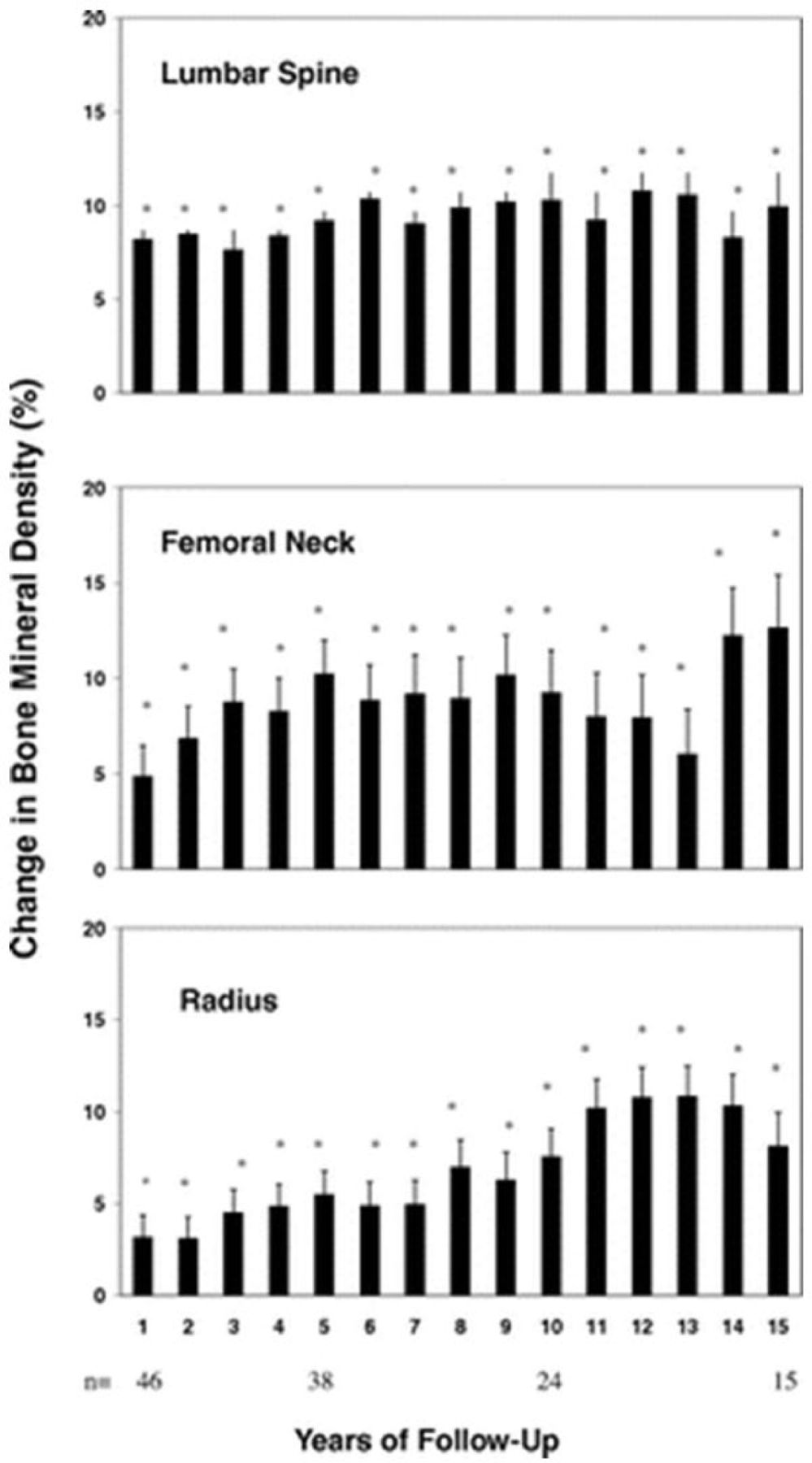
The levels of PTH return to normal after successful parathyroid surgery, and other biochemical indices improve, including calcium, 25-OH and 1,25-OH vitamin D, urinary calcium, and markers of bone resorption and formation. An observational study of 116 patients showed that bone density increased at the lumbar spine, femoral neck, and distal radius after parathyroid surgery (Figure 2) [Rubin MR et al. J Clin Endocrinol Metab 2008].

Improvements in Bone Density After Parathyroid Surgery
*p < .05, compared with baseline.
Reproduced from Rubin MR et al. The Natural History of Primary Hyperparathyroidism with or without Parathyroid Surgery after 15 Years. J Clin Endocrinol Metab. September 2008;93(9):3462–3470. With permission from The Endocrine Society.
MEDICAL MANAGEMENT OF PHPT
Observation is one element of the medical management of PHPT. An observational study of the natural history of PHPT showed that 37% of the asymptomatic patients developed ≥ 1 indication (hypercalcemia, hypercalciuria, or reduced bone mineral density [BMD]) for parathyroid surgery during a 15-year period [Rubin MR et al. J Clin Endocrinol Metab 2008]. The natural history of biochemical indices for PHPT in patients who did not have surgery is shown in Table 1.
Evolution in Biochemical Indices in PHPT During a 15-Year Period
Pharmacological treatment in PHPT includes cinacalcet plus bisphosphonates in patients with severe hypercalcemia and low BMD, or cinacalcet alone for severe hypercalcemia. Several approaches that are not approved by the United States Food and Drug Administration were also mentioned: estrogen plus raloxifene, bisphosphonates alone for low BMD, and denosumab.
Estrogen and raloxifene in combination have been shown to lower serum calcium and have a neutral effect on BMD and PTH. The bisphosphonate alendronate has been shown to have a neutral effect on serum calcium and PTH, and to increase BMD [Khan AA et al. J Clin Endocrinol Metab 2004]. Cinacalcet lowered serum calcium and PTH, and it had a neutral effect on BMD [Peacock M et al. J Clin Endocrinol Metab 2005]. Cinacalcet plus a bisphosphonate were shown to lower serum calcium and PTH, and to increase BMD [Faggiano A et al. Endocrine 2011].
The 2014 Guidelines recommend monitoring of serum calcium annually, as the 2009 Guidelines did [Bilezikian JP et al. J Clin Endocrinol Metab 2009]. The skeletal assessment with DXA every 1 or 2 y is also unchanged, but with the addition of computed tomography or VFA if clinically indicated; renal creatinine clearance assessment is still recommended annually, with the addition of a stone risk profile or abdominal imaging if clinically indicated.
Dr. Bilezikian stated that although the balance of evidence is leaning toward surgery as being the best option for patients with asymptomatic PHPT, both surgical and medical management should be considered for every patient.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.