

Summary
This article outlines the state of health care economics globally and in the United States and offered some reasons why we are often unhappy with our health care system.
- Prevention & Screening
- Prevention & Screening
- Cardiology
- Exclusive Article - For home page
In a keynote address, Uwe Reinhardt, PhD, Princeton University, Princeton, New Jersey, USA, outlined the state of health care economics globally and in the United States and offered some reasons why we are often unhappy with our health care system.
Dr Reinhardt noted that health care is expensive, more so in some countries than in others, particularly the United States. In 2011, Americans spent twice as much on health care compared with any other country. As an example, in other countries the cost of magnetic resonance imaging (MRI) ranges between $118 and $1110; in the United States it costs between $522 and $2900.
When health spending increases, it displaces spending on other desirable things. The things that are given up represent the opportunity costs of added health care spending. These opportunity costs can include reductions in money spent for education, research and development, and infrastructure, less investment in cultural institutions and on internal and external security, as well as giving up things a family might want. One can calculate the net social value added by the health system by subtracting the opportunity costs from the gross value added by health care to patients. For example, between 2011 and 2012 the individual State General Fund spending on Medicaid increased by $15,862 million (based on 2011 data for enacted budgets), while at the same time, the money available for education, public assistance, and transportation decreased (based on 2012 governor-proposed budgets).
Other reasons offered for our dissatisfaction with the US health care system are related to redistribution of cost and perceived inequality of compensation. In most modern countries, well-to-do people pay for the health care of less well-off people. Doctors are sometimes unhappy as they perceive inequality between their input and reward. They help restore health and often save lives, and yet, noted Dr Reinhardt, in general they are paid much less than people in other sectors whose contributions they perceive as having less value. Health care is one of the highest value-added sectors of the economy, because good health is really the most valuable thing to human beings. Although the work can be psychologically rewarding, it is often conducted in an environment full of strife and suspicion. Neither patients nor the public or private insurers who pay on behalf of patients really understand what doctors are doing, thus they often suspect that they are made to pay for unnecessary services.
At the moment, major economic forces are buffeting health care: slower economic growth, rising income inequality, anger at waste in health care, and poor health behavior. Per-capita health care spending grows more quickly when the overall economy is rapidly expanding. We are living in a time when economic growth is slowing, and future growth worldwide is projected to be lower than it has been in past decades. World trade and production have been decreasing since 2010, leading to decreases in gross domestic product (GDP) globally [International Monetary Fund (IMF). World Economic Outlook—Recovery Strengthens, Remains Uneven. Washington, April 2014]. This trend of slower growth is projected to continue out to 2025.
The IMF forecasts that China's inflation-adjusted GDP will continue to slow over the rest of the decade, down to nearly 6% from a high of 10.4% in 2010 [IMF. People's Republic of China. IMF Country Report No. 14/235. 2014]. Between 1965 and 2000, US GDP had an annual growth rate of 2%. Between 2009 and 2013, GDP growth rate was 1.3%. This will result in more pressure on revenues—both through utilization and price pressures, for doctors and other health care providers.
Income inequality is growing worldwide, mainly because of technological change and globalization. In the emerging markets, inequality in income and wealth is particularly pronounced, but it is happening in Europe as well, especially in the United Kingdom. Annual medical costs are increasing rapidly and leading to strains on the average family. In 2001, the medical costs for a typical family of 4 was $8414/y [Milliman, Inc. Milliman Medical Index. 2005]. Today that amount is $23,214, almost 3 times as much [Milliman, Inc. Milliman Medical Index. 2014]. If we look at household median income ($51,017), the difficulty of spending $23,000 on health care becomes obvious [DeNavas-Walt C et al. Income, Poverty, and Health Insurance in the United States: 2012. Washington, DC: US Census Bureau; Current Population Reports, P60-245. 2013]. Thus, the poor are being priced out of health treatment in every country.
Although the US per capita GDP grows by roughly 1.5% per year, the bulk of that growth goes to the bank accounts of the highest top 10% of earners. Although this is a bit less applicable to Europe, the situation is similar in the emerging markets. The contract of social solidarity in health care that had been the dream in most highly developed countries after World War II will be severely tested in the years ahead-especially in the United States. Social solidarity has never existed in the emerging market economies and may never come to life there.
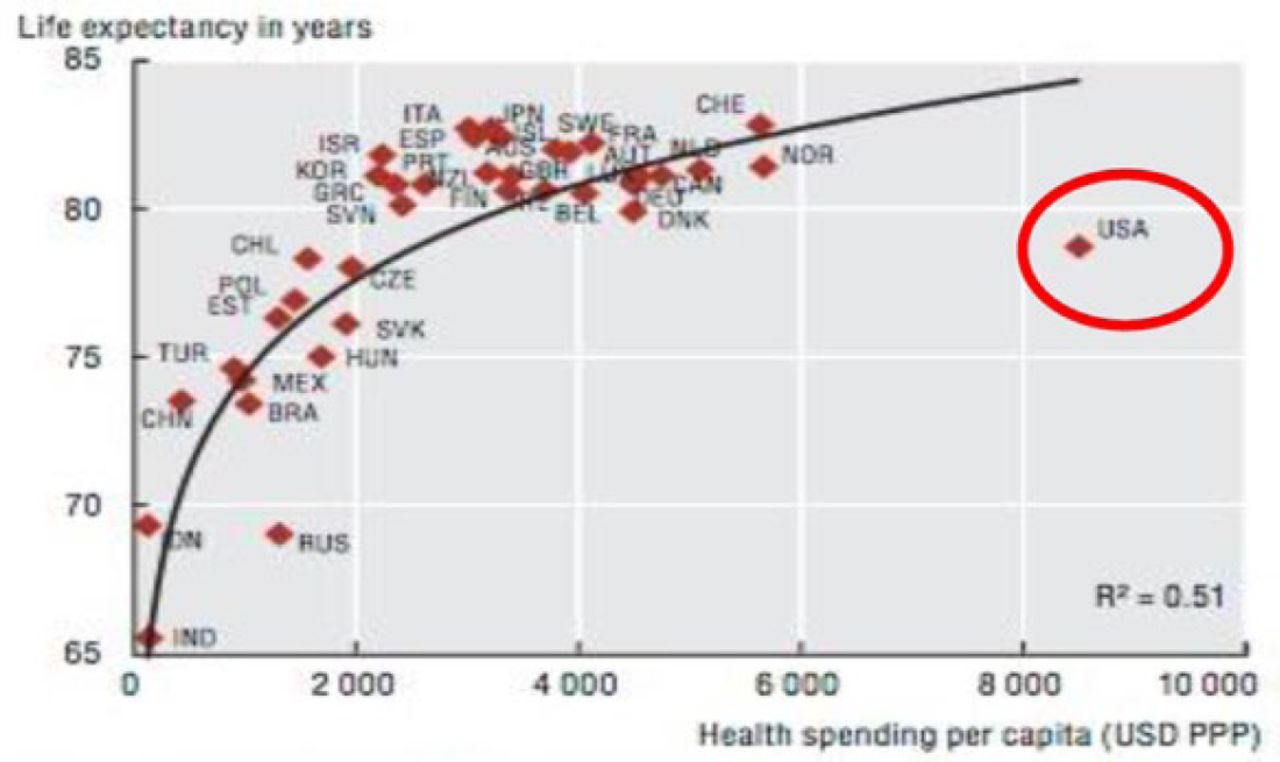
Many are angry with what they see as waste in the health care system. In the United States, we spend more on health care than any other country, but our mean life expectancy is lower than most European countries (Figure 1).

Life Expectancy in Years vs Per Capita Health Care Spending by Country
Reproduced from OECD (2013), Health at a Glance 2013: OECD Indicators, OECD Publishing. http://dx.doi.org/10.1787/health_glance-2013-en. With permission from OECD Publishing.
In 2009, it was estimated that 31% of total health care spending ($2.5 trillion) in the United States was waste (Table 1) [Institute of Medicine (IOM). The Healthcare Imperative: Lowering Costs and Improving Outcomes: Workshop Series Summary. Washington, DC: The National Academies Press, 2010]. This included unnecessary services, inefficiently delivered services, and excess administrative costs, which alone amounted to $190 billion. These administrative costs account for 25.3% of total US hospital expenditures, significantly higher than any other country [Himmelstein DU et al. Health Aff (Millwood). 2014].
Sources of Estimated Excess Costs: United States 2009
Reducing US per capita spending for hospital administration to Scottish or Canadian levels could save more than $150 billion (2011 dollars) with a simpler and less market-oriented payment scheme [Himmelstein DU et al. Health Aff (Millwood). 2014]. This money could then be repurposed for medical innovations and other long-term benefits.
The United States is among the wealthiest nations in the world, but our life expectancy and health status lag behind those in other high-income countries, even though we spend more per person on health care than any other nation [National Research Council and Institute of Medicine. Woolf SH, Aron L, Eds. U.S. Health in International Perspective: Shorter Lives, Poorer Health. Washington, DC: The National Academies Press, 2013]. Poor health behavior among US adults is a major factor in the paradox between the amount spent on health care and outcomes. For example, the percentage of US adults who are obese or who had diagnosed diabetes increased dramatically between 1994 and 2010 [Centers for Disease Control and Prevention (CDC). Diabetes Public Health Resource. http://www.cdc.gov/diabetes/statistics/comp/fig7_overweight.htm. Accessed October 2, 2014].
Dr Reinhardt concluded that, while poor health behavior actually contributes to the increase of health care income, no doctors want their patients to be unhealthy. Health care consumption is important when determining the health status of any nation and consumption can be affected by many factors including the economic status of its people, the environment, and the educational system.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.