

Summary
Patients with psoriasis are at an increased risk of developing multiple comorbidities, including psoriatic arthritis (PsA), cardiovascular disease, diabetes mellitus, and cancer. This article discusses the practical aspects of diagnosing and managing patients, cardiometabolic risk assessment in patients with psoriasis, as well as systemic comorbidities with psoriasis.
- Skin Diseases
- Skin Diseases
- Dermatology
Patients with psoriasis are at an increased risk of developing multiple comorbidities, including psoriatic arthritis (PsA), cardiovascular disease, diabetes mellitus, and cancer. Wolf-Henning Boehncke, MD, MA, University of Geneva, Geneva, Switzerland, discussed the practical aspects of diagnosing and managing patients with psoriasis for dermatologists.
Psoriasis is associated with an increased risk of multiple comorbidities, including obesity, anxiety and depression, diabetes mellitus, and lymphoma, as well as PsA [Daudén E et al. Actas Dermosifiliogr. 2012]. Importantly, up to 42% of patients with psoriasis have PsA, and 75% of patients develop PsA after their diagnosis of plaque psoriasis; therefore, dermatologists serve as sentinels for early detection of the disease. Currently used questionnaires, the Psoriasis Epidemiology Screening Tool, Psoriatic Arthritis Screening and Evaluation, and Toronto Psoriatic Arthritis Screening, may have limited sensitivity for the identification of inflammatory joint disease [Haroon M et al. Ann Rheum Dis. 2013]. Until better screening methods are developed, however, Prof Boehncke suggested that dermatologists continue using screening questionnaires, as well as asking about and examining the patient for tender or swollen joints and back pain. The early diagnosis of PsA is important because a delay of even 6 months is associated with poor functional and radiographic outcomes [Haroon M et al. Ann Rheum Dis. 2014].
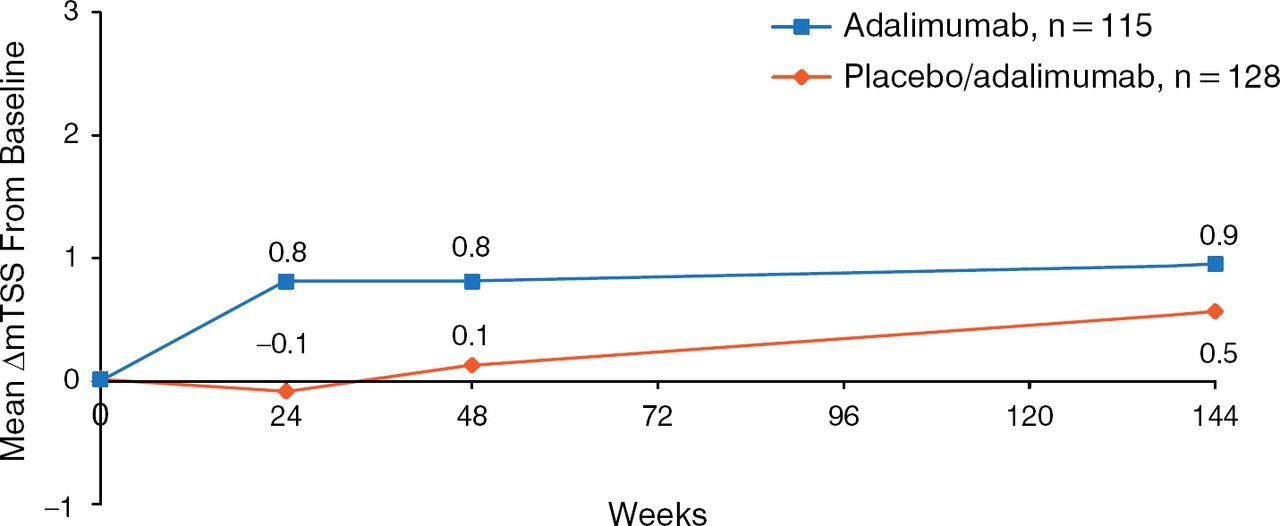
The diagnosis of PsA is important because it affects treatment decisions and generally indicates a need to refer the patient to a rheumatologist. Available treatments include nonsteroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs), and anti-tumor necrosis factor (TNF) therapies. NSAIDs and the currently used DMARDs do not, however, prevent radiographic progression of PsA, whereas anti-TNF therapies, including adalimumab [Mease PJ et al. Ann Rheum Dis. 2009], etanercept, and infliximab, can halt progression (Figure 1).

Anti-Tumor Necrosis Factor Therapies Halt Radiographic Progression of Psoriatic Arthritis
mTSS, modified total Sharp score.
Reproduced with permission from WH Boehncke, MD, MA.
Treatment method can also affect outcomes, because a treat-to-target strategy resulted in nearly 100% of patients who achieved minimal disease activity (MDA) experiencing no radiologic progression, compared with about 35% and 42% of those who did not achieve MDA experiencing radiographic progression at weeks 52 and 104 (P = .012) [Coates LC, Helliwell PS. Arthritis Care Res (Hoboken). 2010].
Nehal Mehta, MD, National Heart, Lung, and Blood Institute, Bethesda, Maryland, USA, outlined the role of cardiometabolic risk assessment in patients with psoriasis. Cardiometabolic disease encompasses the presence of any disease of the vasculature, glucose metabolism, and adipose dysfunction such as obesity, and lipoprotein metabolism. Typically, cardiovascular risk assessment is performed using the Framingham risk score, which predicts the 10-year risk of major adverse cardiovascular events (MACEs) [Wilson PWF et al. Circulation. 1998]. The Framingham risk score, however, does not account for important risk factors such as genetic predisposition, hemostatic or thrombotic disease, behavioral or lifestyle factors other than smoking, and inflammatory disease.
The presence of inflammatory disease, which includes psoriasis, is a risk factor for cardiovascular disease; high-sensitivity C-reactive protein is associated with a relative risk of > 4.0 for future cardiovascular events [Libby P et al. Am J Med. 2004]. In addition, psoriasis is associated with vascular inflammation [Mehta NN et al. Arch Dermatol. 2011]. Patients with severe psoriasis have a 50% increased risk of mortality related to cardiovascular disease and are at an increased risk of developing myocardial infarction and stroke (Table 1) [Maradit-Kremers H et al. Int J Dermatol. 2013; Mehta NN et al. Am J Med. 2011; Mehta NN et al. Eur Heart J. 2010; Gelfand JM et al. J Invest Dermatol. 2009; Gelfand JM et al. JAMA. 2006].
Effect of Severe Psoriasis on Risk of Cardiovascular Disease
Dr Mehta recommends calculating the risk of cardiovascular disease associated with severe psoriasis, by multiplying the adjusted hazard ratio of cardiovascular disease for severe psoriasis (1.531297) by the baseline incidence (0.0115902 events per year), which equals the adjusted incidence rate for severe psoriasis (0.017748) [Mehta NN et al. Am J Med. 2011]. Then, the baseline incidence (0.0115902) can be subtracted from the adjusted incidence rate (0.017748) to equal the excess rate per year (0.006158). The excess rate multiplied by 10 years results in a 10-year risk of 6.2%. Therefore, the Framingham risk score can be adjusted to include the risk of cardiovascular disease associated with psoriasis [Mehta NN et al. J Am Acad Dermatol. 2012]. There is growing support for the idea that all patients with psoriasis should be screened by any health care provider for cardiovascular risk factors beginning at age 18 years and continued every 5 years.
Diamant Thaçi, MD, University of Lübeck, Lübeck, Germany, discussed the association of other systemic comorbidities with psoriasis. Psoriasis has a reported association with Crohn disease [Skroza N et al. Biomed Res Int. 2013]. In addition, patients with psoriasis are at a greater risk of developing celiac disease (odds ratio, 2.36; 95% CI, 1.15 to 4.83) [Bhatia BK et al. J Am Acad Dermatol. 2014].
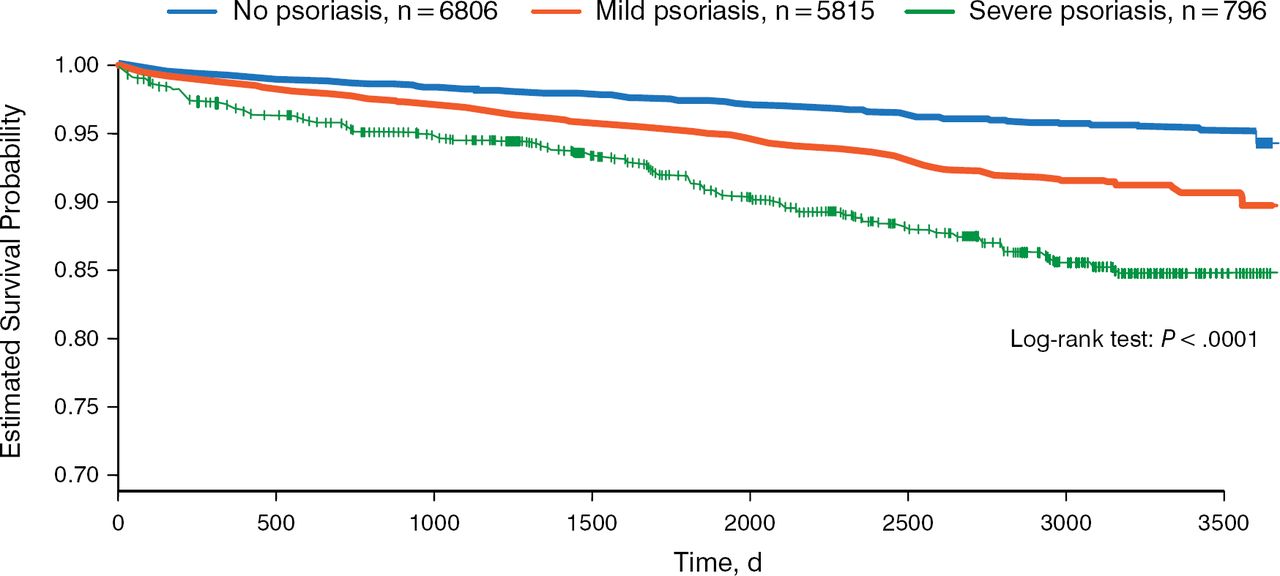
The risk of developing diabetes is also higher in patients with psoriasis [Armstrong AW et al. JAMA Dermatol. 2013], and the Psoriasis Area and Severity Index score is associated with insulin resistance [Boehncke S et al. Br J Dermatol. 2007]. Furthermore, the greater the severity of psoriasis, the shorter the time to the occurrence of diabetes (Figure 2) [Lee MS et al. J Am Acad Dermatol. 2014]. Patients with psoriasis who also have dyslipidemia, hypertension, or Cushing disease may be at an even greater risk of developing diabetes. In addition, treatment of psoriasis with psoralen plus ultraviolet A treatment also appears to increase the risk of diabetes [Lee MS et al. J Am Acad Dermatol. 2014].

Association of Psoriasis Severity and Diabetes Mellitus
Republished with permission of American Academy of Dermatology, from J Am Acad Dermatol. Increased risk of diabetes mellitus in relation to the severity of psoriasis, concomitant medication, and comorbidity: A nationwide population-based cohort study. Lee MS et al. 70(4):691–698. 2014; permission conveyed through Copyright Clearance Center, Inc.
Sleep disturbance is also associated with psoriasis, and treatment with etanercept has been reported to result in improved sleep [Thaçi D et al. J Eur Acad Dermatol Venereol. 2014]. A subanalysis of the PRISTINE study found that patients with moderate to severe psoriasis were more likely to suffer from symptoms of sleep apnea, sleep disturbance, and somnolence compared with the general population. Treatment with etanercept improved these symptoms during a period of 24 weeks.
Data suggest that an elevated risk of cancers, such as those of the colon, bladder, kidney, pharynx, larynx, esophagus, stomach, liver, vulva, breast, and pancreas, as well as leukemia, non-Hodgkin lymphoma, and non-melanoma skin cancers, may be associated with psoriasis, with risk profiles differing for different tumor types [Beyaert R et al. Mol Cancer. 2013].
In conclusion, psoriasis is more than just a disease that affects the skin; psoriasis is associated with serious comorbidities, including inflammatory arthritis, cardiovascular disease, diabetes mellitus, and possibly some cancers. It is important that dermatologists screen for potential comorbidities to initiate early treatment and appropriate referral.

The editors would like to thank the many members of the 2014 European Academy of Dermatology and Venereology presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.