

Summary
Short arm casting with a 3-point molding resulted in improved flexion, supination, and pronation compared with long arm casting in patients with type A2 fractures of the distal radius. Amir R. Kachooei, MD, Mashhad University of Medical Sciences, Mashhad, Iran, presented data from a study [NCT02286661] evaluating the treatment of type A2 fractures of the distal radius by casting.
Short arm casting with a 3-point molding resulted in improved flexion, supination, and pronation compared with long arm casting in patients with type A2 fractures of the distal radius. Amir R. Kachooei, MD, Mashhad University of Medical Sciences, Mashhad, Iran, presented data from a study [NCT02286661] evaluating the treatment of type A2 fractures of the distal radius by casting.
About 17% of fractures are of the distal radius, with about two-thirds requiring surgical treatment; however, initial treatment typically includes closed reduction and immobilization with a plaster cast [Walenkamp MMJ et al. BMC Musculoskelet Disord. 2014]. The purpose of this study was to assess outcomes of 2 different types of casting methods.
In this prospective, multicenter trial, 100 patients with distal radius fractures were randomly assigned to receive a short or long arm cast. All fractures were type A2, and patients with dorsal angulations > 20°, radial shortening > 10 mm, and extensive cortical comminution were excluded. Patients in the short arm cast (SAC) group had their wrist positioned in neutral rotation with volar-ulnar deviation. In the SAC, distal extension of the cast was to the metacarpophalangeal joints dorsally, and to the proximal palmar crease volarly. The cast was extended proximally to 1 inch distal to the antecubital fossa and posteriorly to the olecranon. In the long arm cast (LAC) group, the elbow was positioned in 90° of flexion and the cast was extended to the middle of the arm.
Patients assigned to the LAC group were converted to an SAC at 4 weeks, and all patients had their casts removed at 6 weeks. Reduction failure was defined as > 5 mm displacement or > 5° of angulations. Range of motion was considered abnormal if there was > 10° difference with the unaffected wrist. Baseline, preoperative characteristics including radial inclination in the plain anteroposterior view, dorsal tilt angulations in the lateral view, and radial shortening in the plain anteroposterior view were similar among the SAC and LAC groups.
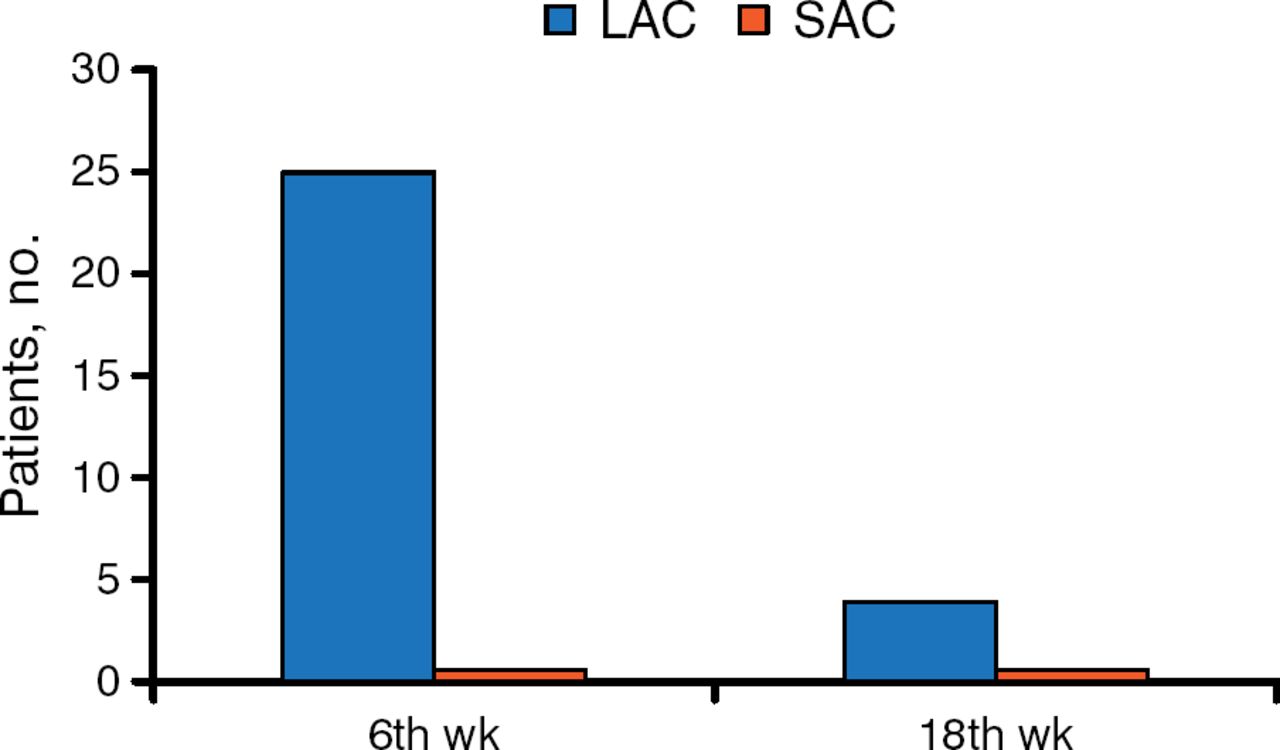
Patients in the SAC group demonstrated greater range of flexion and extension of the elbow at 6 and 18 weeks compared with the LAC group; however, the difference between the groups decreased substantially by the 18th week (Figure 1).

Effect of Casting Type on Elbow Extension
LAC, long arm cast; SAC, short arm cast.
Reproduced with permission from AR Kachooei, MD.
Similarly, patients treated with the SAC experienced greater range of supination and pronation of the forearm at 6 and 18 weeks compared with patients who received the LAC, with the difference between the 2 arms decreasing by week 18. The SAC arm demonstrated fewer blisters and wounds compared with the LAC arm. There was no significant difference in distal radio ulnar joint instability and reduction loss between the 2 arms. Patients reported greater satisfaction with the SAC compared with the LAC. There was no evidence of malunion, nonunion, carpal tunnel syndrome, and compartment syndrome in either group.
Prof Kachooei stated that the data from this study indicate that an SAC with proper 3-point and inter osseous molding provides good therapeutic outcomes in patients with a type A2 fracture.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.