

Summary
This article presents data from an international multicenter study, demonstrating that patients with dual-chamber (DC) implantable cardioverter defibrillators (ICDs) experienced a significantly lower incidence of inappropriate shocks compared with those with single-chamber devices, with no difference in all-cause mortality between the two groups. The Optimal Anti-tachycardia Therapy in ICD Patients Without Pacing Indications study [OPTION; NCT00729703] was designed to test the hypothesis that DC ICD therapy with specific device-based algorithms would reduce the rate of inappropriate shocks without affecting morbidity and mortality by ventricular pacing.
- Interventional Techniques & Devices Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
Christof Kolb, MD, German Heart Centre/Technische Universität München, Munich, Germany, presented data from an international multicenter study, demonstrating that patients with dual-chamber (DC) implantable cardioverter defibrillators (ICDs) experienced a significantly lower incidence of inappropriate shocks compared with those with single-chamber (SC) devices, with no difference in all-cause mortality between the two groups.
Despite its lifesaving potential, ICD therapy remains complicated by inappropriate therapies and shocks that may result in pain, anxiety, depression, and proarrhythmia. Additionally, controversy still exists as to whether a SC or DC device is the most appropriate to prevent inappropriate shocks.
The Optimal Anti-tachycardia Therapy in ICD Patients Without Pacing Indications study [OPTION; NCT00729703] was designed to test the hypothesis that DC ICD therapy with specific device-based algorithms would reduce the rate of inappropriate shocks without affecting morbidity and mortality by ventricular pacing.
OPTION was a prospective, international multicenter trial that was conducted among 54 centers in nine countries in Europe and North America. It enrolled 462 patients (86% men; mean age 63 years; 77% with ischemic heart disease) for 27 months, from 2006 to 2009. Inclusion criteria were implantation of an ICD according to European Society of Cardiology/European Heart Rhythm Association or American College of Cardiology/American Heart Association guidelines, and left ventricular ejection fraction ≤40%.
The primary endpoints of the study were time to first inappropriate shock and percentage of patients with a combined endpoint of all-cause mortality and hospitalization for specified cardiac reasons. Secondary endpoints included occurrence of appropriate and inappropriate shocks, all-cause mortality, and hospitalizations due to cardiovascular (CV) events.
All subjects were supplied with a DC device (Ovatio DR 6550, Sorin Group) and then randomized to undergo SC therapy (SC tachyarrhythmia detection and ventricular back-up pacing at 40 bpm; n=223) or DC therapy (featuring device-based algorithms to reduce the incidence of inappropriate shocks by DC discrimination and to minimize ventricular pacing; n=230).
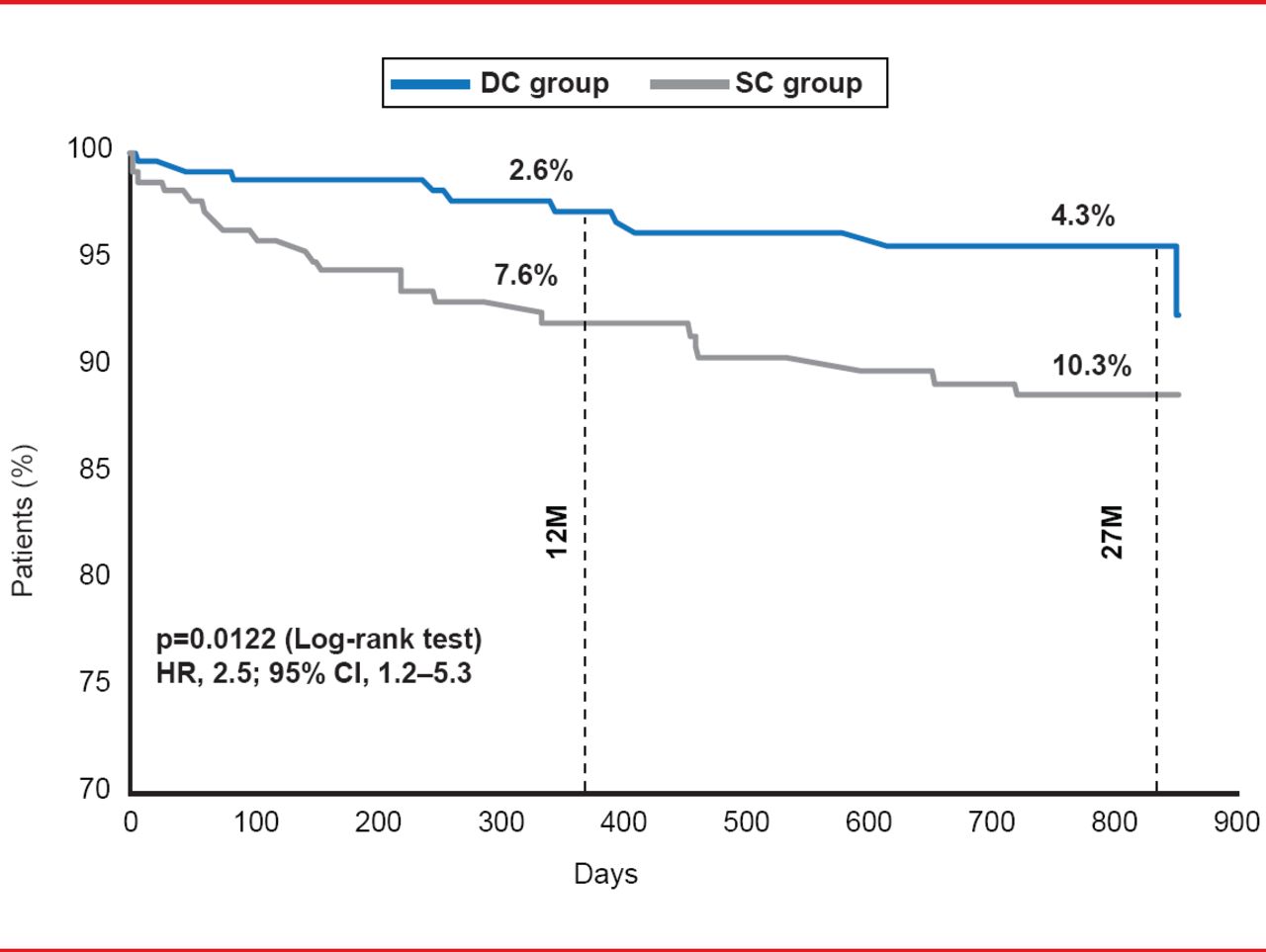
At the study end (27 months follow-up) there was a significant difference in time to first occurrence of inappropriate shock between the two groups, with a significantly lower incidence in the DC arm compared with the SC arm (4.3% vs 10.3%; HR, 2.5; 95% CI, 1.2 to 5.3; log-rank p=0.0122; Figure 1). At 12 months, the incidences were 2.6% and 7.6%, respectively.

Time to First Inappropriate Shock
Reproduced with permission from C Kolb, MD.
Considering the safety aspect, there was no significant difference in mortality and CV events between the two groups. Twenty-one and 18 patients died in the DC and SC groups, respectively, with CV events reported in 33 and 40 patients respectively. Additionally there were relatively few device-related complications overall, with atrial lead complications in 0.9% and 1.8% of patients in the DC and SC groups, respectively.
The investigators concluded that DC ICD therapy resulted in a significantly reduced incidence of inappropriate shocks compared with SC therapy, and similar rates of all-cause mortality and CV events with a low rate of atrial lead complications.
Although further studies may be required to confirm this benefit, the data suggest that when a lower rate of inappropriate shocks is needed, use of a DC ICD is preferable.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.