

Summary
A physiological diagnostic (PhD) algorithm in a cardiac resynchronization device called Paradym (Paradym CRT+PhD) has a low sensitivity of 34% and a false-positive rate of 2.4 per patient year. This article reports on the results the trial Evaluation of a Diagnostic Feature in a Cardiac Resynchronization Therapy Device [CLEPSYDRA; NCT00957541]. A subanalysis of the study provided the basis for development of an alternative device-derived risk stratifier of heart failure (HF) events, identifying patients likely to develop HF decompensation in the following month with a Hazard Ratio of 4.4 [Gold M et al. EuroPace 2013 (abstr P1511)].
- Cardiology Clinical Trials
- Heart Failure
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Heart Failure
- Interventional Techniques & Devices
A physiological diagnostic (PhD) algorithm in a cardiac resynchronization device called Paradym (Paradym CRT+PhD) has a low sensitivity of 34% and a false-positive rate of 2.4 per patient year. Francisco Leyva, MD, University of Birmingham, Birmingham, United Kingdom, reported on the results the trial Evaluation of a Diagnostic Feature in a Cardiac Resynchronization Therapy (CRT) Device [CLEPSYDRA; NCT00957541]. A subanalysis of the study provided the basis for development of an alternative device-derived risk stratifier of heart failure (HF) events, identifying patients likely to develop HF decompensation in the following month with a Hazard Ratio of 4.4 [Gold M et al. EuroPace 2013 (abstr P1511)].
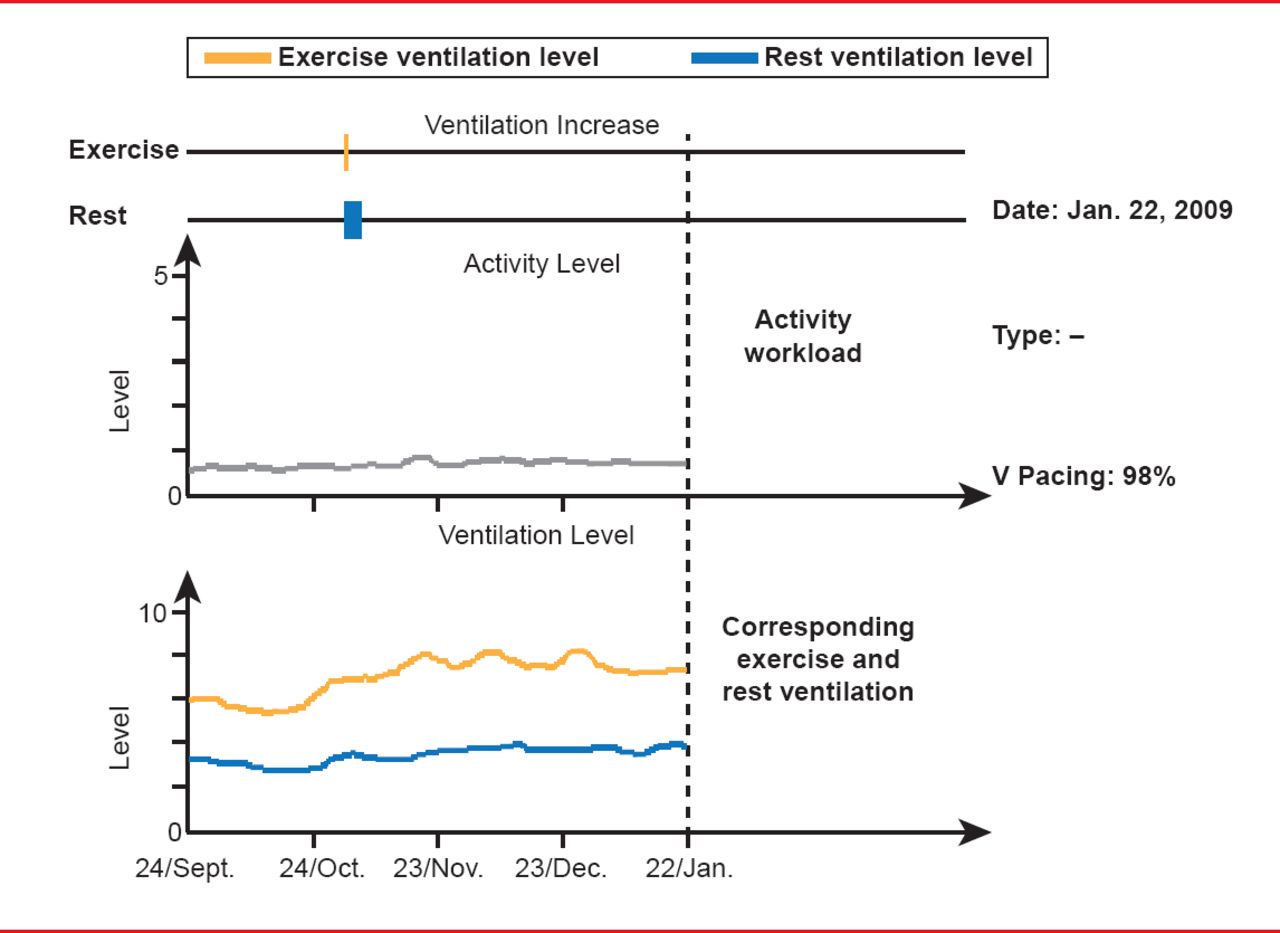
The HF patient journey has a difficult trajectory with frequent hospital admissions [Cleland JG et al. J Am Coll Cardiol 2006], and nothing has been made available to use to predict whether patients would succumb to their disease or return to a more stable path, said Prof. Leyva. But now thoracic impedance can be measured in minute-ventilation (MV=amplitude/period) through a sensor incorporated in the CRT device. From device readings, daily and weekly averages of activity workload and ventilation can be calculated (Figure 1).

Paradym CRT+PhD: Mode of Operation
Reproduced with permission from F Leyva, MD.
In this trial researchers sought to determine the sensitivity of the Paradym CRT+PhD algorithm in detecting potential HF deaths or HF hospitalizations. Since daily activity workloads can change dramatically from day to day, the researchers compared weekly average workloads. Comparing the weekly average on 1 day with the weekly average for the same day a week later can reveal if a condition is worsening or improving.
Eligible patients included those with an HF-related event within 6 months proceeding September 2009, when enrollment began. Eligible patient characteristics were NYHA category III/IV, QRS ≥120 ms, and left ventricular ejection fraction (LVEF) ≤35%. A total of 521 patients were enrolled by April 2011 at centers worldwide: 40 in Europe, 20 in the United States, and 3 in Canada. Baseline characteristics included mean age of 67.4 years, 82% male, QRS 155.3±26.6 ms, and LVEF 25.7%±7.6%. Comorbidities included hypertension and diabetes, 87.1% were taking angiotensin-converting-enzyme inhibitors or angiotensin II receptor blockers, and 87.3% were taking β-blockers.
Sixty-six all-cause deaths occurred during the study (15 HF); 127 patients either died (for all cause) or were hospitalized for HF; and 98 patients experienced either HF death or HF hospitalization (Table 1). The Paradym CRT PhD algorithm had 37 true-positives, 1065 false-positives, and 72 false-negatives, for a false-positive rate of 2.4 per patient-year and a sensitivity of 34%. The most lead-related adverse events observed were 41 (7.9%) diaphragmatic stimulations and 38 (7.5%) LV lead dislodgements. The most procedure-related adverse events included 17 (3.3%) pocket infections and 12 (2.4%) pocket hematomas.
Clinical Outcomes of CLEPSYDRA
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.