

Summary
Atrial fibrillation (AF), the most common cardiac arrhythmia, is associated with a 5-fold increased risk of stroke. Strokes related to AF are more severe and result in greater morbidity and mortality than strokes from other causes. This article reviews the historic role that vitamin K antagonists, particularly warfarin, have had in reducing the risk of stroke associated with AF.
- Cerebrovascular Disease
- Arrhythmias
- Cerebrovascular Disease
- Arrhythmias
- Cardiology
Atrial fibrillation (AF), the most common cardiac arrhythmia, is associated with a 5-fold increased risk of stroke. Strokes related to AF are more severe and result in greater morbidity and mortality than strokes from other causes. Alexander Turpie, MD, McMaster University, Hamilton, Ontario, Canada, reviewed the historic role that vitamin K antagonists (VKAs), particularly warfarin, have had in reducing the risk of stroke associated with AF. Problems with older anticoagulants (eg, delayed onset and offset of action, unpredictable dose-response, narrow therapeutic index, and numerous interactions with food and drugs) have led to many patients not receiving needed therapy. In addition, the requirement for regular monitoring and a high risk of intracranial hemorrhage have been especially problematic.
As the population ages, the number of individuals with AF at risk of stroke is increasing. The problems associated with VKAs have resulted in the need for the development of new agents which do not require as close of monitoring. Dr. Turpie reviewed the development of new oral anticoagulant (NOAC) therapies and compared the features of the NOACs with those of warfarin (Table 1).
Comparison Overview of NOACs With Warfarin
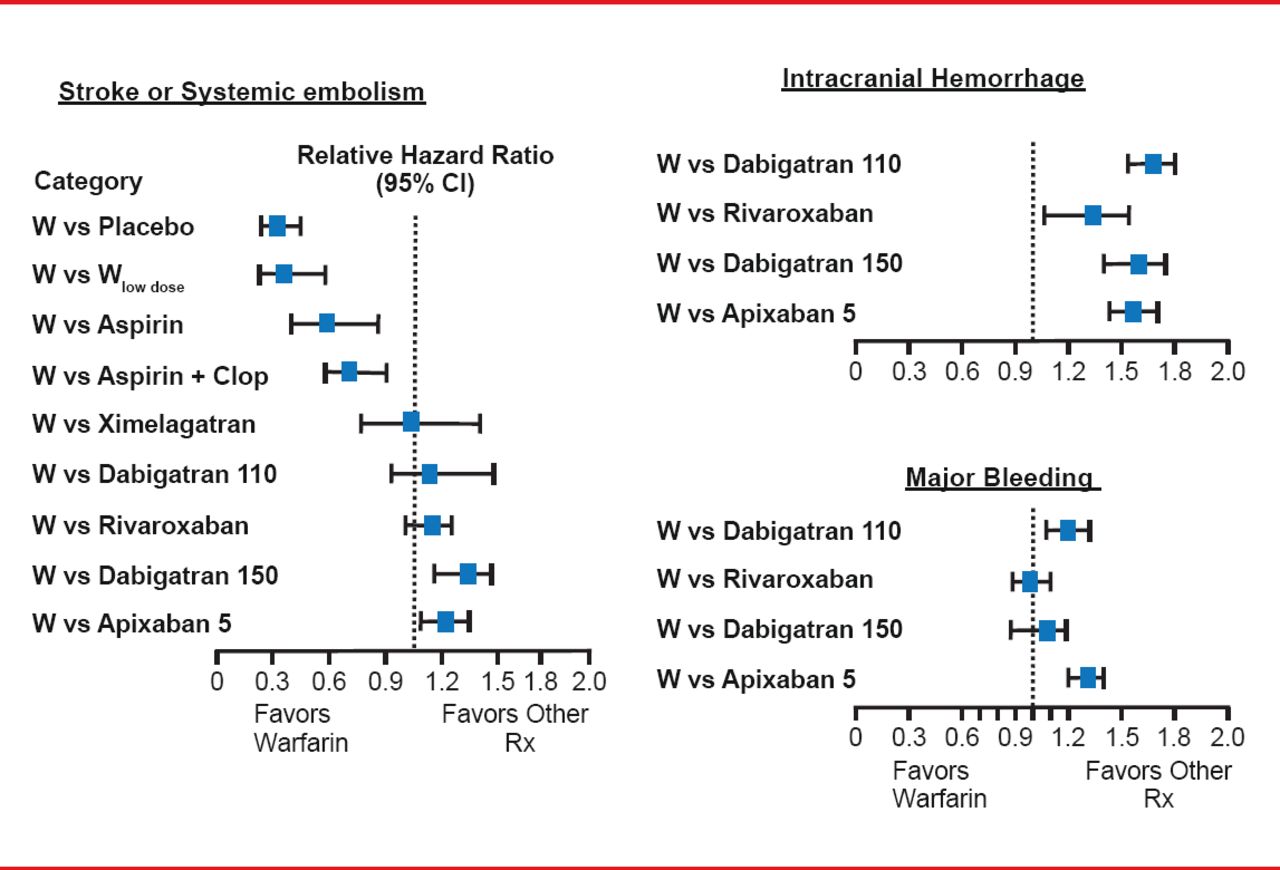
NOACs include the drugs which prevent thrombosis through factor Xa inhibition (rivaroxaban, apixaban, and edoxaban) and direct thrombin inhibitors (dabigatran) [Eikelboom JW, Weitz JI. Circulation 2010]. Clinical trials of NOACs found that these drugs have similar or improved efficacy in reducing stroke or systemic embolization and a lower incidence of intracranial hemorrhage when compared with warfarin (Figure 1) [Granger CB et al. N Engl J Med 2011; Patel MR et al. N Engl J Med 2011; Connolly SJ et al. N Engl J Med 2009].

Stroke Prevention: Oral Anticoagulant Effect
Reproduced with permission from A Turpie, MD.
Noting that the trials of these agents had different designs, included patients with different risk factors, and had slightly different endpoint definitions, Dr. Turpie does not believe that the current clinical trials provide evidence that allows one to compare the individual NOACs. Of the current guidelines for treating patients with AF, Dr. Turpie prefers the guideline from the European Society of Cardiology, updated in 2012 [Camm AJ et al. Eur Heart J 2012]. The three new important points these guidelines make are 1) assess stroke risk exclusively with CHA2DS2-VASc in preference to CHADS2; 2) administer anticoagulation for stroke prevention with a CHA2DS2-VASc score of ≥1; and 3) if anticoagulant therapy is indicated, one of the novel nonmonitored drugs apixaban, rivaroxaban, or dabigatran should be used in preference to VKAs.
Although NOACs do not require monitoring, the activated partial thromboplastin time can be used qualitatively for patients on dabigatran and the prothrombin time for patients on rivaroxaban [Heidbuchel H et al. Europace 2012; Mani H et al. Thromb Hemost 2011]. This may provide useful in formation where suspected overdosage or lack of adherence is suspected, and for patients with renal insufficiency or extreme body weight. All anticoagulant drugs cause bleeding, and the lack of an antidote for the new agents has been mentioned as a drawback. Dr. Turpie said that bleeding should be managed by discontinuing the drug, providing fluid resuscitation, applying pressure on the bleeding site if exposed, and giving recombinant factor VIIa or prothrombin complex concentrates for ongoing life-threatening bleeding. Dabigatran is cleared primarily by the kidney [Elkeboom JW, Weitz JI. Circulation 2010], requiring more careful management that includes routine monitoring of renal function in patients with reduced creatinine clearance.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.