

Summary
Despite high levels of compliance with antiplatelet and statin medications, the proportion of middle aged, East Asian patients who meet guideline recommended cardiovascular disease (CVD) management targets prior to catheterization is suboptimal. This article reports the results of a prospective study designed to determine whether patients referred for a coronary angiogram or percutaneous coronary intervention (PCI) at a single center in the West Indies were meeting guideline recommended CVD management targets.
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
Despite high levels of compliance with antiplatelet and statin medications, the proportion of middle aged, East Asian patients who meet guideline recommended cardiovascular disease (CVD) management targets prior to catheterization is suboptimal, reported Godfrey Aleong, MD, FESC, Eric Williams Medical Science Complex, Trinidad, West Indies.
CVD is the number one cause of death in Trinidad and Tobago. The large burden of disease is associated with long waits for, and limited access to, coronary angiography. Dr. Aleong reported the results of a prospective study designed to determine whether patients referred for a coronary angiogram or percutaneous coronary intervention (PCI) at a single center in the West Indies were meeting guideline recommended CVD management targets.
The investigators collected data on characteristics and medications in 41 patients, as well as lifestyle advice (dietary and exercise), and the following parameters of CVD management:
-
▪ Body mass index (BMI; <24.9 kg/m2)
-
▪ Blood pressure (BP; nondiabetics <140/90 mm Hg; diabetics <130/80 mm Hg)
-
▪ Heart rate (<70 bpm after 5 minutes in a supine position)
-
▪ Fasting LDL <70 mg/dL
-
▪ Fasting glucose <130 mg/dL and HbA1C <7.0% for diabetic patients
Subjects had a mean age of 57.1±9.3 years, and the majority were men (82.9%). More than 80% were East Asian. The risk factors for CVD included current or past smoker (46.3% of subjects), a diagnosis of diabetes (26.8%), hypertension (41.5%), dyslipidemia (31.7%), and/or a family history of premature coronary artery disease (41.5%). A majority of the patients had a history of myocardial infarction (68.3%). Almost all subjects reported angina (92.7%); approximately two thirds (68.3%) had dyspnea.
Nearly all subjects (97%) were on antiplatelet therapy (aspirin 87.8%; clopidogrel 78.0%). Approximately two thirds of patients were taking β-blockers (65.9%). All subjects were on statins (100.0%) and the most commonly used statin was simvastatin (65.9%). More than three quarters of subjects were on either an angiotensin-converting-enzyme inhibitor (84.4%) or an angiotensin II receptor blocker (15.6%). More than half of the subjects (53.7%) were on a proton pump inhibitor.
Of those receiving dietary (n=18) or exercise (n=21) advice, 57.9% and 47.6% were compliant, respectively. Among subjects with diabetes (n=11), 63.6% had a BMI of <24.9 kg/m2 and 54.5% had a fasting glucose <130 mg/dL. In the diabetic population, 63.6% followed advice on regular blood sugar monitoring (Table 1).
Proportion of Subjects (n=41) Achieving Target
The investigators hypothesized that the low rate of subjects achieving the target LDL of <70 mg/dL may be attributable to the large proportion of subjects receiving simvastatin (65.9%), a less potent lipid-lowering drug. The use of lifestyle advice (diet or exercise), which ranged between 40% and 50%, was low and may reflect the large volume of patients seen in the public sector clinics. Despite adequate prescribing, the proportion of patients in this study who achieved guideline targets was suboptimal.
PCI AND SAME-DAY DISCHARGE
Most patients undergoing PCI remain in the hospital overnight to be monitored for postprocedural complications such as myocardial infarction, bleeding, acute stent thrombosis, and renal failure. However, InterQual criteria have now classified elective PCI as an outpatient procedure. Since the Centers for Medicare and Medicaid Services use the InterQual criteria to determine inappropriate admissions related to 1-day inpatient stays and reimbursement rates, hospitals are now working to shift uncomplicated PCI surgery to be classified as same-day discharge (SDD).
Candidates for SDD should have stable vital signs, no cardiac chest pain, a stable vascular access site, be taking oral medications, and have an initial supply of dual antiplatelet therapy. Howard Bush, MD, Cleveland Clinic Florida, Weston, Florida, presented evidence suggesting that increased utilization of the transradial approach for PCI may increase the likelihood of being able to discharge post-PCI patients on the same day. Cardiac catheterization using a radial approach offers several advantages: improved patient comfort, avoidance of prolonged bed rest, shorter postprocedural hospital stays, lower cost, and reduction/avoidance of access site bleeding complications.
In a multicenter cohort study of 107,018 patients aged >65 years who underwent PCI, SDD, although rarely implemented (prevalence 1.25%), was not associated with a greater risk of 2-day death or rehospitalization compared with overnight observation (0.37%; 95% CI, 0.16 to 0.87 vs 0.50%; 95% CI, 0.46 to 0.54; p=0.51) [Rao SV et al. JAMA 2011].
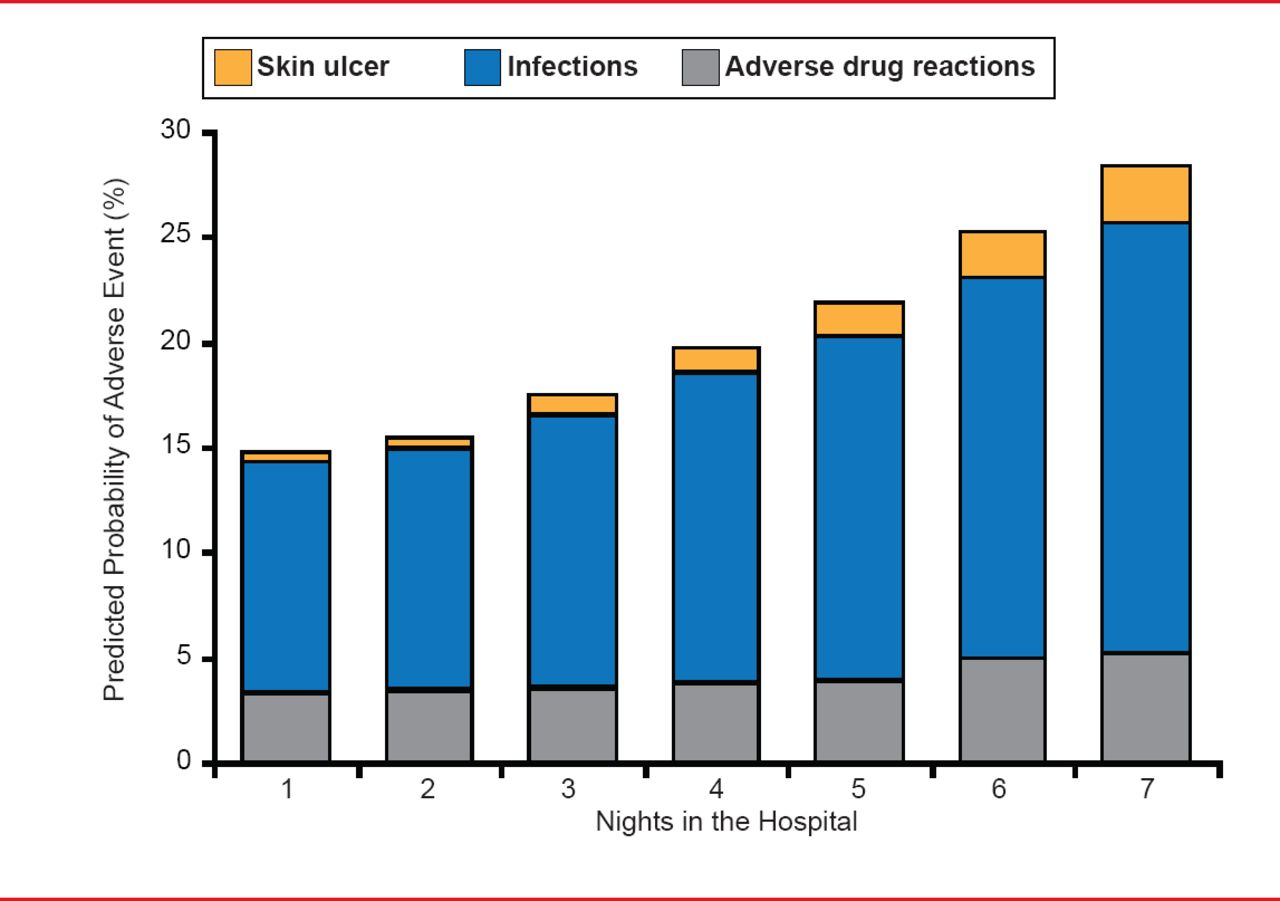
In the Early Discharge After Transradial Stenting of Coronary Arteries trial [EASY; Rinfret S et al. J Am Coll Cardiol Intv 2010], the mean post-PCI hospital stay was significantly shorter (p<0.001) for outpatients (8.9 hours) versus overnight-stay patients (26.5 hours). At 30-day follow-up, the outpatient PCI group achieved an ∼50% savings in post-PCI costs, due mostly to the extra cost of the overnight stay. Hospital stays also carry the added risk of adverse drug reactions, infection, and skin ulcers (Figure 1). Each additional night in the hospital increases the risk by 0.5% for adverse drug reactions, 1.6% for infections, and 0.5% for ulcers [Hauck K and Zhao X. Med Care 2011].

Hazards of Hospitalization
Reproduced with permission from H Bush, MD.
Acceptance of SDD as standard protocol among hospitals and cardiologists has been slow. There is a pressing need for large-scale randomized clinical trials to provide specific evidence-based guidelines. In a recent editorial, Eltigani Abdelaal, MD, and Olivier F. Bertrand, MD, PhD, of the Quebec Heart & Lung Institute, proposed seven essential components of a safe and successful outpatient program [Abdelaal E, Bertrand OF. Catheter Cardiovasc Interv 2013].
The benefits of SDD lie in the potential to reduce procedural costs, increase hospital efficiency, and improve patient satisfaction related to the avoidance of an overnight hospital stay. SDD could potentially open up beds for other inpatient admissions in hospitals operating at near maximal capacity. A strategy that shifts uncomplicated PCI to SDD has become a priority to better align hospital resource utilization with payer expectations.

The editors would like to thank the many members of the Caribbean Cardiac Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Cited By...
- No citing articles found.