

Summary
Persons with type 2 diabetes mellitus, especially the obese, tend to have more visceral fat than persons with type 1 [Gallager D et al. Am J Clin Nutr 2009]. The hallmarks of diabetes are obesity and weight gain, mainly involving abdominal fat, and approaches to addressing these are discussed in this article. Other topics include the targeting low-density lipoprotein cholesterol (LDL-C) and waist circumference and the risk of cardiovascular disease.
- Exclusive Article - For home page
- Cardiometabolic Disorder
- Diabetes Mellitus
- Obesity
- Exclusive Article - For home page
- Endocrinology
- Diabetes & Metabolic Syndrome
- Diabetes Mellitus
- Obesity
- Cardiometabolic Disorder
The hallmarks of diabetes are obesity and weight gain, mainly involving abdominal fat, and approaches to addressing these were discussed by Luc Van Gaal, MD, PhD, Antwerp University Hospital, Antwerp, Belgium. Persons with type 2 diabetes mellitus (T2DM), especially the obese, tend to have more visceral fat than persons with type 1 [Gallagher D et al. Am J Clin Nutr 2009]. Conventional treatments of diabetes typically produce weight gain over time involving subcutaneous and visceral fat [UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; Kahn SE et al. N Engl J Med 2006].
Therapeutic weight control studies in patients with T2DM have assessed sulfonylurea, thiazolidinediones, insulin, metformin, dipeptidyl peptidase-4 inhibitors, and glucagon-like peptide-1 (GLP-1) receptor agonists. Weight loss has been documented only for metformin (50% of cases) and GLP-1 receptor agonists [Drucker DJ. J Clin Invest 2007].
Diet and aerobic exercise are beneficial in reducing visceral fat [Després JP et al. Am J Physiol 1991; Ross R et al. Ann Intern Med 2000; Christiansen T et al. Eur J Endocrinol 2009]. Resistance exercise also reduces visceral fat and intrahepatic lipids [Lee S et al. Diabetes 2012]. Aerobic and resistance exercise also reduces body weight and waist circumference in older individuals [Davidson LE et al. Arch Intern Med 2009]. Even without weight loss, exercise increases skeletal muscle mass, cardiorespiratory fitness, and insulin sensitivity [Ross R, Bradshaw AJ. Nat Rev Endocrinol 2009].
Oral drug therapy for weight and abdominal fat control in diabetes includes topiramate plus phentermine, and lipase inhibition (orlistat). Despite the weight lowering effects of sibutramine [Van Gaal LF et al. Int J Obes Relat Metab Disord 1998], concerns about the increased risk of adverse cardiovascular (CV) events [James WP et al. N Engl J Med 2010] have prevented approval in some countries.
Second-generation peripheral CB1 antagonists, 11β hydroxysteroid dehydrogenase inhibitor, growth hormone in lipodystrophy, GLP-1 analogues (liraglutide, exenatide), SGLT-2 inhibitors (dapagliflozin), and leptin plus pramlintide are novel medications being studied to reduce intra-abdominal fat.
TARGETING LDL-C
Kwang Kon Koh, MD, PhD, Gachon University Gil Medical Center, Incheon, South Korea, discussed targeting low-density lipoprotein cholesterol (LDL-C) in patients with abdominal obesity.
Patients with hypertension and diabetes are at increased risk of CV events. Long-term survival is also significantly decreased compared to patients without diabetes [Verdecchia P et al. Hypertension 2004]. Thus preventing the development of diabetes is an important treatment goal.
Visceral fat is a hallmark of obesity and may drive inflammation and insulin resistance. In turn, this increases the risk of hypertension, T2DM, and dyslipidemia. These important risk factors increase the risk of developing atherosclerosis and cardiovascular disease (CVD) [Lim S et al. Circ J 2011; Koh KK et al. Int J Cardiol 2012].
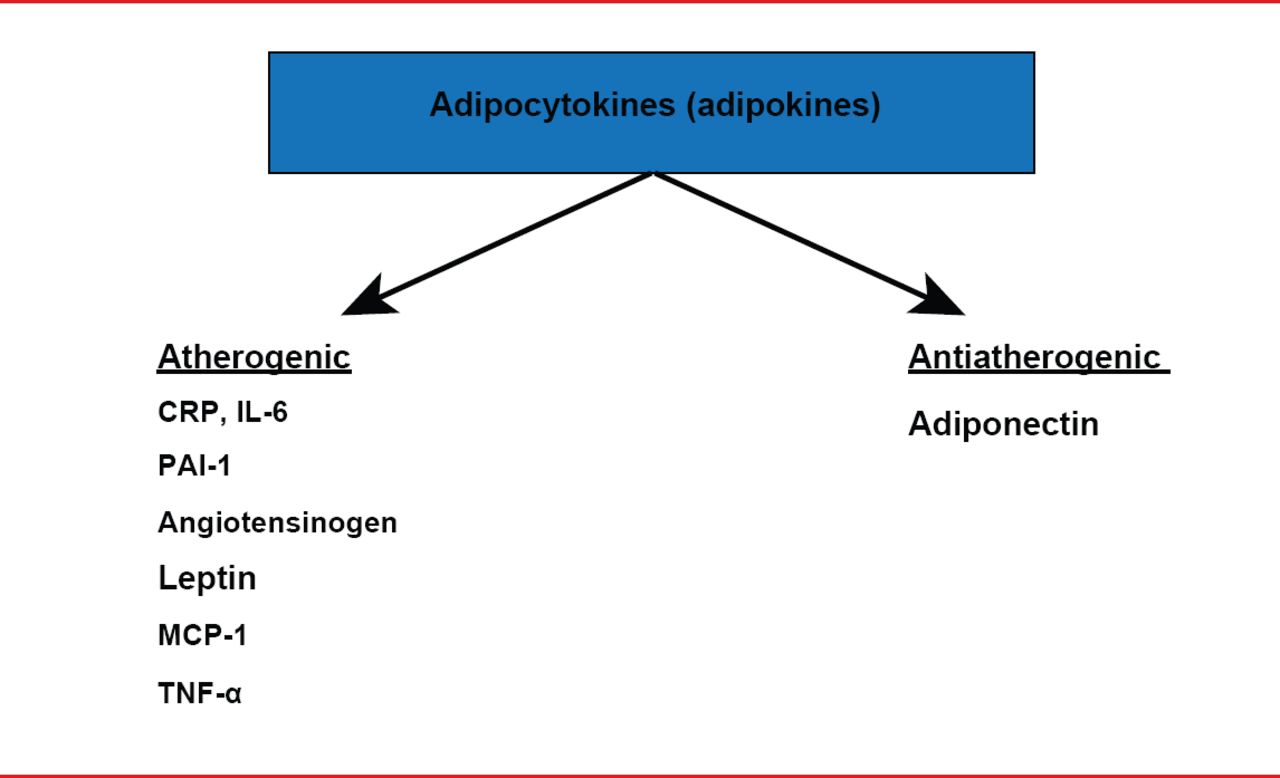
Adipocytes produce bioactive molecules that participate in diverse metabolic processes [Lau DC et al. Am J Physiol Heart Circ Physiol 2005; Wellen KE, Hotamisligil GS. J Clin Invest 2005] (Figure 1). With increasing visceral adipose mass, adiponectin secretion decreases and the secretion of adipokines that reduce insulin sensitivity and contribute to endothelial dysfunction is increased. Thus, obesity and T2DM heighten CV risk.

Adipose Tissue as an Endrocrine Organ
CRP=C-reactive protein; IL-6=interleukin-6; MCP-1=monocyte chemoattractant protein-1; PAI-1=plasminogen activator inhibitor-1; TNF-α=tumor necrosis factor-alpha
Simvastatin lowers adiponectin and reduces insulin sensitivity in patients with hypercholesterolemia [Koh KK et al. Diabetes Care 2008], while atorvastatin and rosuvastatin increase glucose and insulin sensitivity in such patients [Koh KK et al. J Am Coll Cardiol 2010; Koh KK et al. Int J Cardiol 2013]. Atorvastatin and rosuvastatin mildly increase the risk of diabetes [Sattar N et al. Lancet 2010; Goldstein MR, Mascitelli L. Curr Diab Rep 2013].
However, insulin resistance and endothelial dysfunction are both subject to multiple influences. Interactions between insulin resistance and endothelial function may mediate the pathophysiology of conditions such as diabetes, obesity, dyslipidemia, coronary artery disease, hypertension, and atherosclerosis [Mora S et al. Circulation 2012]. Combined statin-based therapy has shown promise in improving oxidative stress [Koh KK et al. Circulation 2004], altering levels of triglycerides and high-density lipoprotein cholesterol, and increasing insulin sensitivity [Koh KK et al. Hypertension 2005; Koh KK et al. J Am Coll Cardiol 2005].
Thus, despite the concerns about an increase risk of diabetes with use of potent statins, they have a central role in the primary and secondary prevention of coronary heart disease (CHD), in concert with modifiable lifestyle changes, stated Prof. Koh (Table 1).
Practical Recommendations for Statin Choice
HYPERTRIGLYCERIDEMIC WAIST AND CARDIOMETABOLIC RISK
Benoit Arsenault, PhD, Université Laval, Québec City, Québec, Canada, discussed waist circumference and the risk of CVD.
Myocardial infarction risk increases with increasing body mass index (BMI) and waist circumference [Yusuf S et al. Lancet 2005]. Visceral, but not subcutaneous adiposity, is associated with adverse CV events [Britton KA et al. J Am Coll Cardiol 2013].
Studies have indicated the importance of the hypertriglyceridemic (HyperTG) waist phenotype — the combination of increased waist circumference and elevated triglycerides — for prediction of cardiometabolic risk and associated CVD risk. The relationship between visceral fat and increased coronary artery calcium score in HyperTG waist patients with T2DM has been described [Sam S et al. Diabetes Care 2009], as has the increased risk of coronary heart disease [Arsenault BJ et al. Can Med Assoc J 2010]. In the latter study, the HyperTG waist phenotype was associated with the most precipitous decline in probability of event-free survival.
The collective findings have led to a number of conclusions and recommendations (Table 2).
Important Aspects of the HyperTG Waist
GLOBAL CARDIOMETABOLIC APPROACH ORGANIZATION AS A MODEL
Denis Richard, PhD, Université Laval, Québec City, Québec, Canada, reviewed the Canadian network for research in cardiometabolic health, diabetes, and obesity (CMDO).
The prevalence of obesity in Canada has increased from almost 15% in 1979 to nearly 25% in 2008. Canada ranks among the top nations globally in terms of national prevalence of diabetes, which, for Canadians aged 35 to 39 years and 40 to 44 years has increased from 1.5% and 2% respectively in 1998, to 2.5% and 4% respectively in 2008. Thirty three percent of Canadians die of diabetes-related causes annually.
The CMDO network comprises research silos of cardiometabolic health, diabetes, and obesity. The CMDO network emphasizes basic and preclinical research, nutrition, physical activity, human physiopathology, lifestyle habits, population health, health care delivery and policy and knowledge dissemination/exchange.
As CMDO strives to move away from a silo-based approach, long-term collaborative research will be needed to study the association of cardiometabolic health, diabetes, and obesity with respiratory diseases and cancer [Boulet LP. Clin Exp Allergy 2013] [Gilbert CA, Slingerland JM. Ann Rev Med 2013].
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.