

Summary
In 2010, the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) proposed new classification criteria for rheumatoid arthritis [Aletaha D et al. Arthritis Rheum 2010]. These criteria were developed with the objective that they would facilitate the identification of subjects in earlier stages of disease. This article discusses the 2010 criteria and their impact on clinical practice.
- Exclusive Article - For home page Guidelines
- Rheumatoid Arthritis
- Featured Meeting - Specialty page
In 2010, the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) proposed new classification criteria for rheumatoid arthritis (RA) [Aletaha D et al. Arthritis Rheum 2010]. These criteria were developed with the objective that they would facilitate the identification of subjects in earlier stages of disease. Following is a summary of 2 presentations from a session that was devoted to a discussion of the 2010 criteria and their impact on clinical practice.
Julia Nicolau, MD, Rouen University Hospital, Rouen, France, discussed a study conducted at her institution that aimed to validate the new criteria in an independent community-based very early arthritis cohort (VErA). The validation was accomplished by comparing the performance of the new criteria against the 1987 ACR classification for the identification of RA [Arnett FC et al. Arthritis Rheum 1988]. Results of the study indicated that in this VErA cohort, the 2010 ACR/EULAR criteria classified slightly more patients as having RA than the 1987 ACR criteria, but otherwise, they performed similarly.
The VErA cohort comprised 310 patients aged ≥18 years, with ≥2 swollen joints that persisted for at least 4 weeks but less than 6 months. All subjects were naïve to treatment with disease-modifying antirheumatic drugs (DMARDs) and steroids and received conservative treatment for the first 2 years. The demographics of the overall population are shown in Table 1.
Overall Population (n=301).
The objective of the study was to compare the diagnostic performance of the 2010 criteria with modification of the erosion item either by excluding it or changing the erosion threshold from 1 to 3. For both objectives, 2 gold standards were used: expert diagnosis at 6 years and the presence of ≥3 erosions at 2 years. Diagnosis was made by the consensus of a panel of 3 experts using patients' files that contained no data concerning treatment or prior ACR classification. Radiographs were read centrally by 2 experienced rheumatologists. Only “significant” erosion (Sharp-van der Heijde score ≥1) was considered. After applying the algorithm, 41 patients were determined not to have RA. Forty of the remaining 269 patients had evidence of ≥1 erosion. When the scoring system for the 2010 criteria was applied to the remaining 229 subjects, 142 were diagnosed with RA and 87 were diagnosed with undifferentiated arthritis.
At baseline, 67.7% of subjects fulfilled the 2010 ACR/EULAR criteria, and 59.3% fulfilled the 1987 ACR criteria (McNemar's test 0.01). When using the expert diagnosis as gold standard, the sensitivity of the ACR/EULAR 2010 criteria was significantly higher than that of the 1987 ACR criteria but with similar specificity. When the cutoff point for typical rheumatoid erosions was modified from ≥1 to ≥3, the sensitivity was similar, but the specificity was significantly higher. The results were comparable when the erosion step was excluded. When using ≥3 erosions at 2 years as the gold standard, the performance of the 2 sets of criteria was similar. The discriminative ability of strict application of the 2010 ACR/EULAR and 1987 ACR criteria was comparable, with areas under the curve (AUC) of 0.76 and 0.79, respectively. The AUC of the ACR/EULAR criteria, without taking the erosion status into consideration, was significantly higher than the strict application of the AUC of the criteria: 0.82 versus 0.76 (Table 2).
Comparison of Criteria Using Expert Diagnosis at 6 Years as the Gold Standard.
Receiver operating characteristic (ROC) curves showed that a score ≥6, proposed by the 2010 criteria for the classification of definite RA, was relevant. Application of the score after excluding a diagnosis of “another rheumatism,” without considering the “erosions” item of the algorithm, provided better performance than the strict application of 2010 ACR/EULAR criteria.
The 2010 ACR/EULAR RA classification criteria refer to a possible use of ultrasonography to confirm clinical findings; however, the exact method to confirm the presence of synovitis with ultrasound has not been reported. Daiki Nakagomi, MD, Chiba University Hospital, Chiba, Japan, discussed the results of a study that aimed to determine the optimized definition of ultrasound synovitis for the 2010 ACR/EULAR criteria and assess the impact of its use on the accuracy of the RA classification.
The study analyzed 107 patients with musculoskeletal symptoms for ≤3 years that could not be explained by diseases other than RA. Patients underwent full assessment, including a systematic multiplanar gray-scale (GS) and Power Doppler (PD) ultrasound examination, which was performed on 38 joint regions at baseline. All patients received routine care from expert rheumatologists who were blinded to the ultrasound findings. A semiquantitative scoring system (0 to 3) was used for both GS synovitis and PD signal. The gold standard that was used in the process of developing the 2010 ACR/EULAR criteria (ie, methotrexate treatment within the first year) was used, and the association between criteria fulfillment at baseline and methotrexate treatment within the first year was analyzed. Patient demographics are shown in Table 3.
Patient Demographics and Joint Manifestations at Baseline.
To compare ultrasound findings with clinical findings, the investigators tentatively identified 2 definitions of ultrasound synovitis: GS score ≥1 or PD score ≥1 (GS≥1/PD≥1) and GS score ≥2 or PD score ≥1 (GS≥2/PD≥1). The prevalence of GS≥1/PD≥1 synovitis was higher than that of clinical synovitis in most joint lesions, with significant differences in wrist (p<0.001), knee (p<0.001), and metatarsophalangeal joints (p<0.01). However, prevalence of GS≥1/PD≥1 synovitis was significantly lower than clinical synovitis in proximal interphalangeal joints (p<0.001). The prevalence of GS≥2/PD≥1 synovitis was lower than that of clinical synovitis in most joint regions.
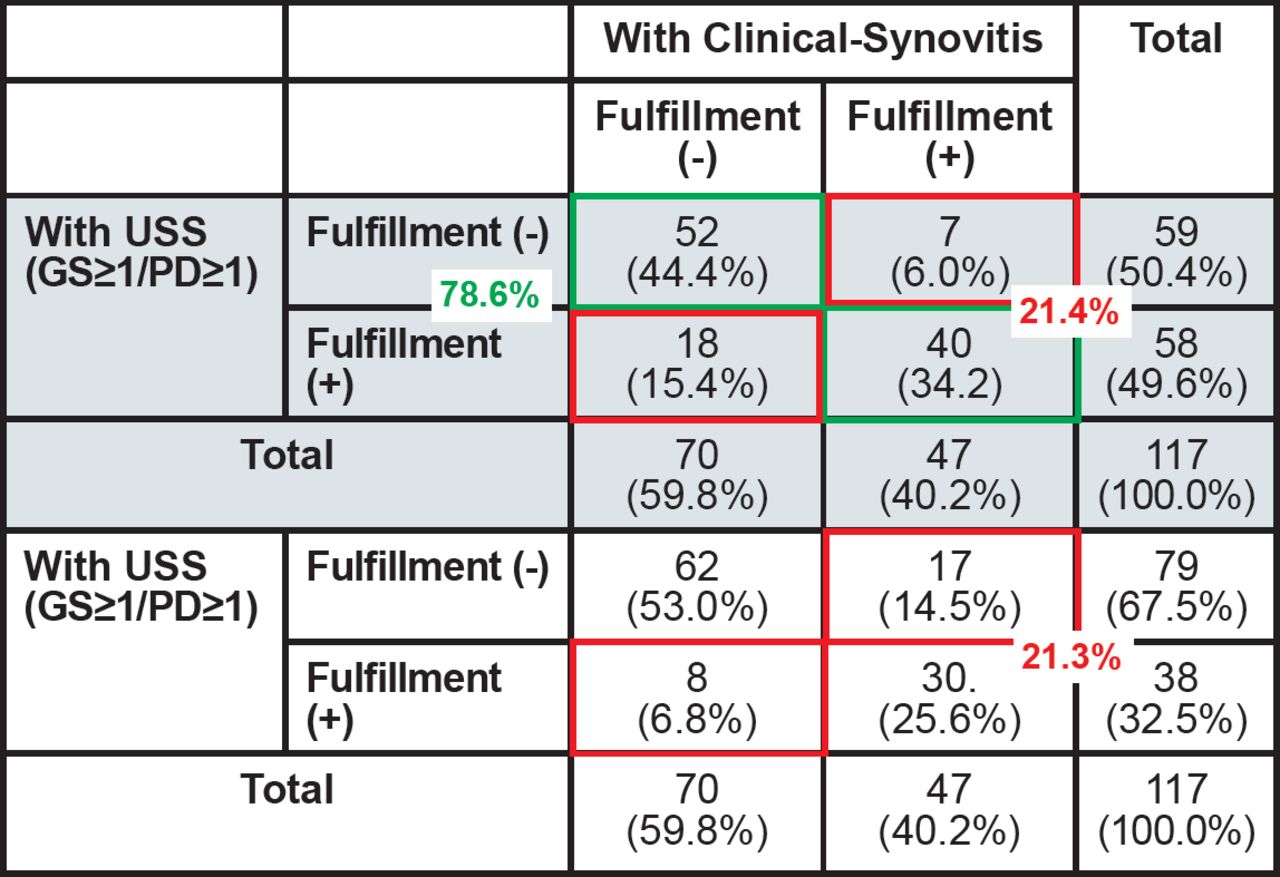
When the requirement for joint swelling and joint count in the 2010 criteria was replaced with the GS≥1/PD≥1 definition of ultrasound synovitis, 78.6% of patients maintained the same classification, 15.4% who did not fulfill the criteria without ultrasound were reclassified to RA, and 6% of patients were reclassified from RA to non-RA. When the GS≥2/PD≥1 definition for ultrasound synovitis was applied, even more cases were reclassified from RA to non-RA. The proportion of patients who were reclassified by using ultrasound was ∼20% with either definition (Figure 1).

Number of Cases Fulfilling the 2010 ACR/EULAR RA Classification Criteria Using Clinical or Ultrasound Assessment.
USS=ultrasound-synovitis; GS=gray scale; PD=power Doppler.
The proportion of patients who developed a disease that required treatment with methotrexate within 1 year was significantly higher among those who fulfilled the criteria with clinical synovitis versus those who did not. The proportion was even larger, however, when ultrasound synovitis was utilized.
The sensitivity and specificity of the 2010 criteria without ultrasound in predicting a requirement for methotrexate within the first year of classification were 63.3% and 79.4%, respectively. When GS≥1/PD≥1 ultrasound synovitis was applied, the sensitivity increased to 81.6%, and when GS≥2/PD≥1 definition was applied, the specificity increased markedly to 93.7%.
ROC analysis demonstrated the largest AUC for the criteria score with GS≥2/PD≥1 ultrasound synovitis, followed by with GS≥1/PD≥1 ultrasound synovitis and without ultrasound.
These results show that ultrasound assessment of synovitis improves the accuracy of the criteria to predict methotrexate requirement, and both definitions can be useful, depending on the purpose of classification.

The editors would like to thank the many members of the European League Against Rheumatism presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.