

Summary
Glycemic management in type 2 diabetes mellitus (T2DM) has become increasingly complex and, to some extent, controversial. A widening array of pharmacological agents [Nyenwe EA et al. Metabolism 2011; Blonde L. Am J Med 2010; Bergenstal RM et al. Am J Med 2010] has raised concerns about their potential adverse effects, as well as new uncertainties about the effects of intensive glycemic control on macrovascular complications [Yudkin JS et al. Lancet 2011]. This article reviews key points from the new Position Statement from the American Diabetes Association and the European Association for the Study of Diabetes [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
- Prevention & Screening
- Hyperglycemia/Hypoglycemia
- Diabetes Mellitus
- Nursing
- Diabetes & Endocrinology Guidelines
Overview
Glycemic management in type 2 diabetes mellitus (T2DM) has become increasingly complex and, to some extent, controversial. A widening array of pharmacological agents [Nyenwe EA et al. Metabolism 2011; Blonde L. Am J Med 2010; Bergenstal RM et al. Am J Med 2010] has raised concerns about their potential adverse effects, as well as new uncertainties about the effects of intensive glycemic control on macrovascular complications [Yudkin JS et al. Lancet 2011]. Many clinicians are, therefore, perplexed as to the optimal treatment strategies for their patients [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
Silvio E. Inzucchi, MD, Yale University School of Medicine, New Haven, Connecticut, USA, reviewed key points from the new Position Statement from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
The statement covers the growing variety and number of antihyperglycemic agents, new data on the benefits versus risks of tight glycemic control, increasing concerns about drug safety, and growing discourse about personalized medicine and patient-centered care. Dr. Inzucchi pointed out that prior guidelines were consensus documents that did not undergo formal Association review to become official position statements.
Main Pathological Defects in T2DM
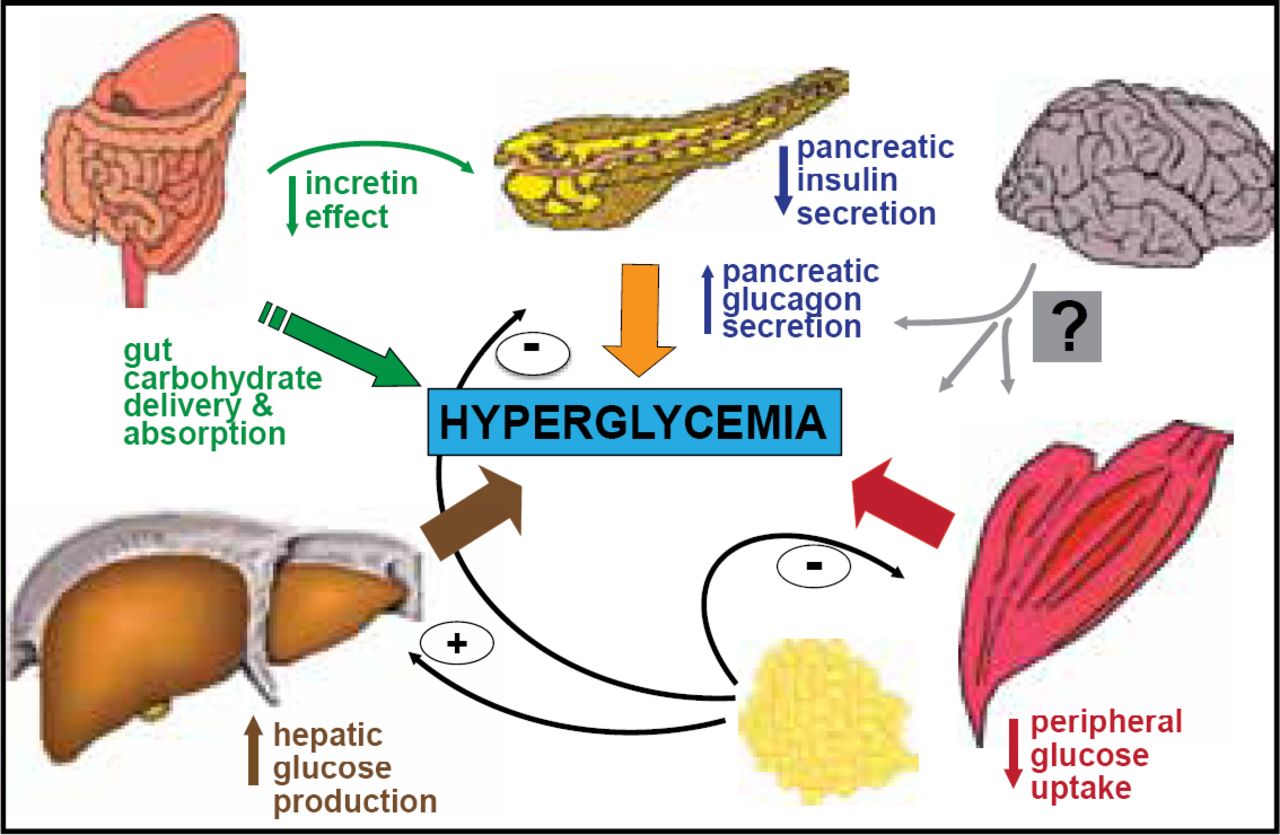
Any rise in glycemia is the net result of glucose influx exceeding glucose outflow from the plasma compartment [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012]. In the fasting state, hyperglycemia is directly related to increased hepatic glucose production. In the postprandial state, further glucose excursions result from the combination of insufficient suppression of this glucose output and defective insulin stimulation of glucose disposal in target tissues, mainly skeletal muscle.
Abnormal islet cell function that progresses over time is a key and requisite feature of T2DM and the main quantitative determinant of hyperglycemia [Ferrannini E et al. J Clin Endocrinol Metab 2005] (Figure 1). However, islet dysfunction is not necessarily irreversible. It responds to increased insulin action that relieves β-cell secretory burden and any intervention that improves glycemia, from energy restriction to bariatric surgery [Ferrannini E. Cell Metab 2010]. More recently, abnormalities in the incretin system have also been identified [Nauck MA. Am J Med 2009].

Main Pathophysiological Defects in T2DM.
Reproduced with permission from SE Inzucchi, MD.
Antihyperglycemic agents are directed at one or more of the pathophysiological defects of T2DM, or they modify physiological processes related to appetite or to nutrient absorption or excretion. Ultimately, T2DM is a disease that is heterogeneous in both its pathogenesis and clinical manifestation. This point must be considered when determining the optimal therapeutic strategy for individual patients [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
Patient-Centered Approach
According to Dr. Inzucchi, patient-centered care is defined as an approach to providing treatment that is respectful of and responsive to an individual patient's preferences, needs, and values, and it ensures that a patient's values guide all clinical decisions [Committee on Quality of Health Care in America: Institute of Medicine. The National Academies Press 2001]. He noted that this should be the organizing principle underlying health care for individuals with any chronic disease, but it is especially pertinent in T2DM, with the uncertainties of choice as well as the sequence of therapy [Inzucchi et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
In a shared decision-making approach, the clinician and the patient act as partners, mutually exchanging information and deliberating on options to reach a consensus on the therapeutic course of action [Tsapas A, Matthews DR. Diabetologia 2008]. Ultimately, the patient makes the final decisions regarding lifestyle choices and, to some degree, the pharmaceutical interventions used [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
A patient's involvement in medical decision-making constitutes one of the core principles of evidence-based medicine, which mandates the synthesis of best available evidence from the literature with the clinician's expertise and the patient's inclination [Guyatt GH et al. JAMA 2000]. The implementation of the plan occurs in the context of a patient's real life and his consumption of public and private resources [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
For many people with complex, chronic comorbidities, the burden of treatment reduces their capacity to collaborate in their care. Therefore, clinicians must establish the weight of burden, encourage coordination in clinical practice, acknowledge comorbidity in clinical evidence, and prioritize from the patient's perspective [May C et al. BMJ 2009].
Position Statement
The document refers to glycemic control pursued within a multifactorial risk-reduction framework. Such a framework is necessary because patients with T2DM are at increased risk of cardiovascular (CV) morbidity and mortality. Aggressive management of CV risk factors (blood pressure and lipid therapy, antiplatelet treatment, and smoking cessation) is likely to have even greater benefits among these patients [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
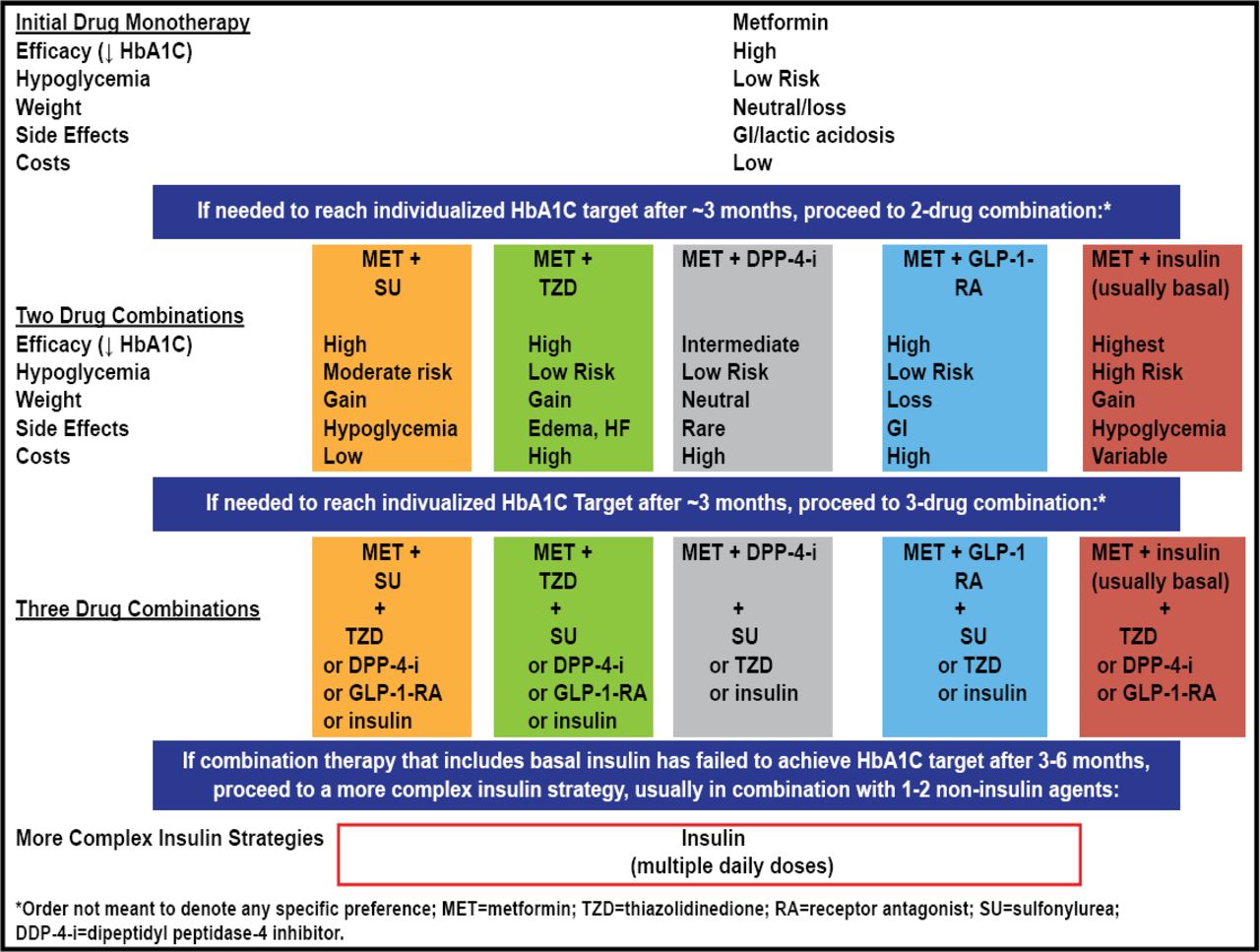
The key points of the ADA/EASD Position Statement: Management of Hyperglycemia in Type 2 Diabetes are: 1) glycemic target blood-glucose lowering therapies must be individualized; 2) diet, exercise, and education are the foundation of any T2DM therapy program; 3) unless contraindicated, metformin is the optimal first-line drug; 4) after metformin, data are limited; combination therapy with one or two other oral/injectable agents that minimize side effects is reasonable; 5) ultimately, many patients will require insulin therapy alone or in combination with other agents to maintain blood glucose control; 6) all treatment decisions should be made in conjunction with the patient (focus on preferences, needs, and values); and 7) comprehensive CV risk reduction is a major focus of therapy [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
Compared with the 2008 ADA/EASD Treatment Algorithm, the 2012 statement is not as prescriptive/algorithmic. It calibrates treatment targets to patients' needs and acknowledges the role of lifestyle change prior to metformin in selected patients. It individualizes treatment options and harmonizes 5 dual-therapy options after metformin. It recognizes the role of initial combination therapy (HbA1C >9%), and endorses triple therapy, when required. It also includes insulin options beyond basal and basal-bolus (Figure 2).

The ADA/EASD Position Statement on Management of Hyperglycemia in T2DM.
Reproduced with permission from SE Inzucchi, MD.
The position statement clearly argues for less stringent HbA1C goals in patients who are predisposed to hyperglycemia and have limited life expectancy, advanced complications, extensive comorbidities, or a glycemic target that is difficult to control despite intensive education, counseling, and effective doses of glucose-lowering agents.
The statement was developed over a period of approximately 2 years by an international writing group, chaired by Dr. Inzucchi and Professor David Matthews from Oxford University and underwent dozens of revisions with additional input from 25 experts around the world. It highlights a proposed patient-centered approach that provides not only the most comprehensive management strategy to date, but also the most vetted and thoroughly reviewed statement ever published [Cefalu CT. Diabetes Care 2012].
It is an expansive approach that suggests recommendations considered within the context of the needs, preferences, and tolerances of each patient. At the same time, the recommendations clearly state that the informed judgment and expertise of experienced clinicians will always be necessary [Cefalu CT. Diabetes Care 2012].
This new ADA/EASD Position Statement will generate a wide range of opinions and emotions. However, no one will disagree with the fact that the initiative was conducted with due diligence deserving of a document that will likely have major impact for millions of patients throughout the world [Cefalu CT. Diabetes Care 2012].
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.