

Summary
This selected update in dyslipidemia discusses the ongoing controversy between fibrate and niacin treatments, as well as the best evidence for lipid-lowering therapy in regards to issues of cardiovascular risk with diabetes. Also discussed is the ongoing question of whether statins cause diabetes.
- Diabetes Mellitus
- Lipid Disorders
Fibrate and Niacin – An Ongoing Controversy
Marshall B. Elam, PhD, MD, University of Tennessee Health Sciences, Memphis, Tennessee, USA, used a case-based approach to discuss controversy surrounding the use of fibrates and niacin to reduce cardiovascular (CV) risk in the age of statins.
Post hoc analyses of cardiovascular disease (CVD) events in dyslipidemic subgroups of major fibrate trials showed significant CVD risk reductions, ranging from 31% (p=0.03) in Action to Control Cardiovascular Risk in Diabetes [ACCORD; NCT00000620] study [Ginsberg HN et al. N Engl J Med 2010] to 78% (p=0.002) in the Helsinki Heart Study [Tenkanen L et al. Circulation 1995] (Table 1). The Fenofibrate Intervention and Event Lowering in Diabetes [FIELD; Keech A et al. Lancet 2005] and ACCORD-Lipid [Ginsberg HN et al. N Engl J Med 2010] substudies also showed renal microvascular benefits from fenofibrate, as well as significant relative percent risk reduction for retinopathy [Chew EY et al. N Engl J Med 2010].
Post Hoc Analyses of CVD Events in Dyslipidemic Subgroups of Major Fibrate Trials.
In May 2011, the Endocrine and Metabolic Drug Advisory Panel of the US Food and Drug Administration (FDA) reviewed the indication for combined fenofibric acid plus statin therapy for dyslipidemia. It found insufficient evidence that adding a fibrate to statin therapy reduces the risk of CVD events in patients with type 2 diabetes and noted the need for a trial to test the hypothesis [Goldfine AB et al. N Engl J Med 2011].
A US Veterans Administration Cooperative study—Fenofibric Acid Intervention to Reduce Residual Risk in Statin-Treated Patients [VA-FIRST] study—has a proposed start date in the fall of 2013. A second new trial, The Fixed Dose Simvastatin + Niacin-ER trial [HPS-Thrive; NCT00461630], is exploring the role of niacin following the Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides: Impact on Global Health Outcomes [AIM HIGH; NCT00880178] trial. Respective outcomes from these studies will help determine the safety and efficacy of fibrates for mixed high-risk primary and secondary prevention and of niacin for additional low-density lipoprotein (LDL)-lowering effect in statin-treated patients.
CV Risk in Patients With Diabetes Mellitus—What Is the Best Evidence for Lipid-Lowering Therapy?
Anne Carol Goldberg, MD, Washington University School of Medicine, St. Louis, Missouri, USA, discussed the status of the Adult Treatment Panel (ATP) IV guideline and major trials that show significant evidence favoring aggressive lipid-lowering treatment to reduce CV risk in people with diabetes.
ATP IV recommendations will reflect evidence from randomized controlled trials of lipid-lowering therapy on CV outcomes as well as high-quality meta-analyses of randomized controlled CV outcomes trials.
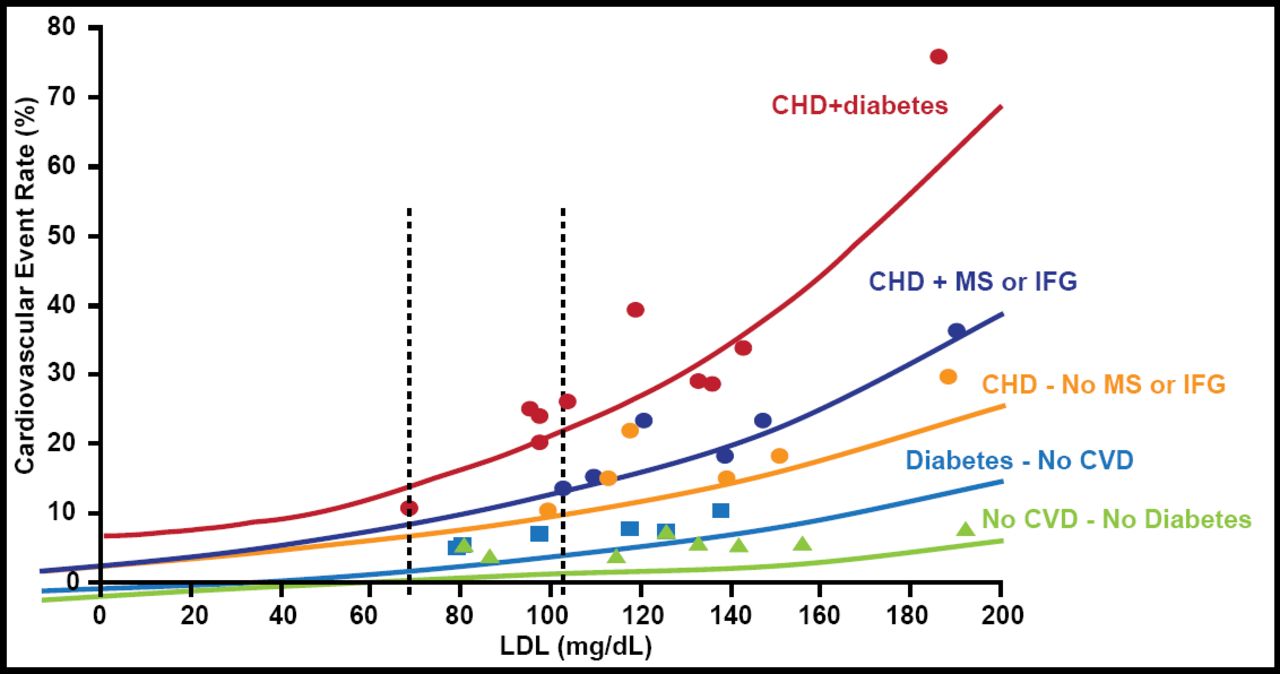
Robinson and Stone [Robinson JG, Stone NJ. Am J Cardiol 2006] used published subgroup analyses from statin event trials to evaluate the relationship between LDL-cholesterol (LDL-C) level and absolute risk of a CV event. Their findings showed that patients with coronary heart disease (CHD) and diabetes had the highest risk (Figure 1).

Relationship Between LDL-C Level and Absolute Risk of a CV Event.
Reproduced with permission from Elsevier. Robinson JG, Stone NJ. Identifying Patients for Aggressive Cholesterol Lowering: The Risk Curve Concept. Am J Cardiol 2006;98(10):1405–1408.
A 2008 meta-analysis by the Cholesterol Treatment Trialists' Collaborators included 14 randomized statin outcomes trials and used individual patient-level analyses in patients with diabetes. Similar effects on CV event reduction were seen in patients with diabetes with and without vascular disease. There was a 21% reduction in major vascular events per 39-mg/dL LDL-C reduction [Cholesterol Treatment Trialists' (CTT) Collaborators. Lancet 2008].
Statins are the evidence-based drugs of choice for primary and secondary CV risk reduction. The CTT Collaboration [Baigent C et al. Lancet 2010] found that further reductions in LDL-C safely produce greater declines in the incidence of heart attack, revascularization, and ischemic stroke. Each 1.0-mmol/L (18-mg/dL) reduction in LDL-C lowers the annual rate of these major vascular events by just over one-fifth. Evidence suggests a 2-mmol/L to 3-mmol/L (36-mg/dL to 54-mg/dL) decrease in LDL-C would reduce risk by 40% to 50%.
Do Statins Cause Diabetes?
Trials of statin therapy have had conflicting findings on the risk of developing diabetes mellitus in patients who are given statins [Sattar N et al. Lancet 2010]. Naveed Sattar, MBChB, MRCP, British Heart Foundation Cardiovascular Research Centre, University of Glasgow, Glasgow, Scotland, United Kingdom, discussed the relationship between statins and diabetes.
According to Prof. Sattar, skeptics of a relationship between statins and incident type 2 diabetes point to nonsignificant associations in trials with glucose data (OR 1.078; 95% CI, 0.97 to 1.17; p=32%); an analysis of 11 trials with biochemical analyses led to null results (p=0.10) and no link to baseline factors [Sattar N et al. Lancet 2010]. However, the body of evidence of an association between statins and incident diabetes mellitus is growing.
In the Stroke Prevention by Aggressive Reduction of Cholesterol [SPARCL; NCT00147602] trial [Waters DD et al. J Am Coll Cardiol 2011; Amarenco P et al. N Engl J Med 2006], Waters et al. found that treatment with 80 mg of atorvastatin led to new-onset diabetes in 166 of 1905 patients versus 115 of 1898 who took placebo (HR, 1.44; 95% CI, 1.14 to 1.83). Researchers also found that the strongest predictors of new-onset type 2 diabetes were baseline fasting glucose and other features of the metabolic syndrome and that the greater the number of risk factors, the higher the risk of developing new-onset type 2 diabetes. There were 9 new cases of diabetes mellitus per 10 patients who were protected from major CVD events—ie, a 44% (95% CI, 14% to 83%) increase in new-onset diabetes mellitus.
In the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin [JUPITER; NCT00239681] trial [Ridker PM et al. N Engl J Med 2008], investigators reported 7 new cases of diabetes mellitus per 10 patients who were protected from major CVD events (myocardial infarction, stroke, CVD death), or a 26% (95% CI, 4% to 51%) increase in new-onset diabetes mellitus. Similarly, in a pooled analysis of data from 5 statin trials, Preiss et al. [Preiss D et al. JAMA 2011] found that intensive-dose statin therapy was associated with an increased risk of new-onset diabetes compared with moderatedose statin therapy. As compared with moderatedose statin therapy, the number needed to harm per year for intensive-dose statin therapy was 498 for new-onset diabetes, while the number needed to treat per year for intensive-dose statin therapy was 155 for CV events.
Given this evidence, the US FDA recently added information to statin labels regarding an effect of these agents on diabetes, noting that “increases in glycosylated hemoglobin (HbA1C) and fasting serum glucose levels have been reported with statin use,” but adding that the “FDA continues to believe that the CV benefits of statins outweigh these small increased risks” [Goldfine AB. N Engl J Med 2012].
Ultimately, statin recommendations will not change, but new data might prompt physicians to measure glucose/HbA1C when considering statins [Sattar N, Preiss D. Diabetologia 2012], warn patients about a slight risk of diabetes mellitus, and use that information as an additional incentive to promote lifestyle changes [Goldfine AB. N Engl J Med 2012].
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.