

Summary
This article discusses the recently introduced anticoagulant, dabigatran, for use in patients with atrial fibrillation (AF). AF is a strong independent risk factor for stroke. However, judicious use of antithrombotic therapy reduces the risk for most patients who have the condition.
- Cerebrovascular Disease
- Arrhythmias
“There has not been this much excitement about an anticoagulation tablet since warfarin was introduced 60 years ago,” said Fady Turquieh, MD, University of Balamand, Al-Kurah, Lebanon, speaking about dabigatran, the recently introduced anticoagulant, for use in patients with atrial fibrillation (AF).
AF is a strong independent risk factor for stroke. However, judicious use of antithrombotic therapy reduces the risk for most patients who have the condition. Warfarin reduces the risk of ischemic and hemorrhagic stroke by 64% in patients with AF (95% CI, 49% to 74%) [Hart RG et al. Ann Intern Med 2007]. Compared with warfarin, dabigatran 150 mg is associated with even lower rates of stroke and systemic embolism (SE) but similar rates of major hemorrhage [Connolly SJ et al. N Engl J Med 2009].
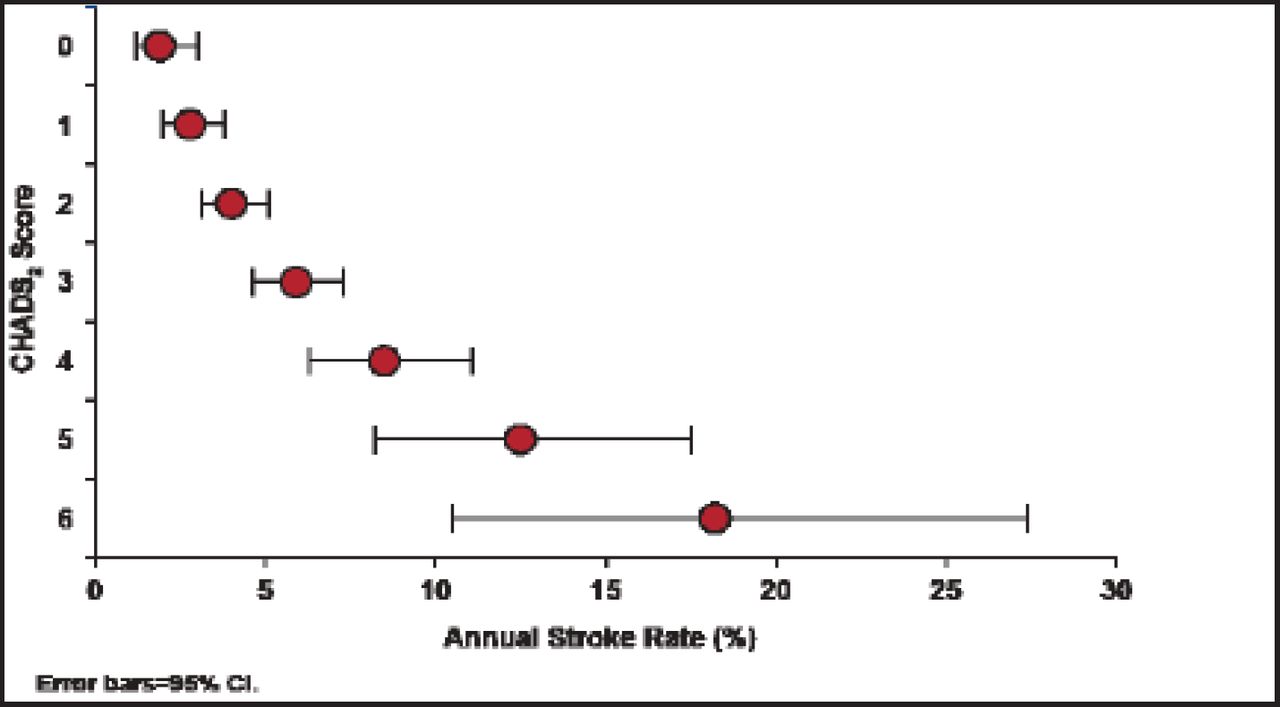
Warfarin, a vitamin K antagonist (VKA), has proven efficacy for various thrombotic diseases. But it also has several important limitations, including variability in response, a narrow therapeutic window, and dietary and drug interactions [Vargas Ruiz AG et al. Gac Med Mex 2012]. Classification schemes, such as the CHADS2 score, can quantify the risk of stroke for patients who have AF, and may aid in the selection of appropriate antithrombotic therapy (Figure 1) [Gage BF et al. JAMA 2001].

Estimation of Stroke Risk in AF Using CHADS2.
Copyright © 2001 American Medical Association. All rights reserved.
In patients with AF taking warfarin, risks of death, myocardial infarction (MI), major bleeding, stroke, and systemic embolism event (SEE) are related to international normalized ratio (INR). Although good control of INR is important to improve clinical outcomes, target INRs are not frequently achieved [White HD et al. Arch Intern Med 2007].
According to Prof. Turquieh, one third to one half of patients who would benefit from anticoagulation therapy do not receive it, and those who do spend a third of their time outside the target INR range; most often they are under- rather than over-anticoagulated.
White et al. [Arch Intern Med 2007] found that patients in the poor INR control group had higher rates of annual mortality (4.2%) and major bleeding (3.85%) compared with the moderate control group (1.84% and 1.96%, respectively) and the good control group (1.69% and 1.58%, respectively; p<0.01 for all). Compared with the good control group, the poor control group had higher rates of MI (1.38% vs 0.62%; p=0.04), and stroke or SEE (2.10% vs 1.07%; p=0.02).
The oral direct thrombin inhibitor dabigatran and oral direct inhibitors of factor Xa (eg, rivaroxaban and apixaban) have recently emerged as potential alternatives to VKAs for stroke prevention in AF. Their advantages are a fixed dosage, no need to monitor coagulation parameters, and fewer interactions with food and other medications [De Caterina R et al. J Am Coll Cardiol 2012].
The primary objective of the Randomized Evaluation of Long-Term Anticoagulant Therapy [RE-LY] study was to establish the noninferiority of dabigatran etexilate to warfarin. The median duration of the follow-up period was 2 years; 18,113 patients who had AF and a risk of stroke participated in the study. They received fixed doses of dabigatran 100 or 150 mg BID in a blinded fashion, or adjusted-dose warfarin in an unblinded fashion. The primary outcome was stroke or SEE [Connolly SJ et al. N Engl J Med 2009].
Rates of the primary outcome were 1.69% per year for those taking warfarin compared with 1.53% per year in the group taking dabigatran 110 mg (RR with dabigatran, 0.91; 95% CI, 0.74 to 1.11; p<0.001 for noninferiority) and 1.11% per year in the group that received dabigatran 150 mg (RR, 0.66; 95% CI, 0.53 to 0.82; p<0.001 for superiority).
The rate of major bleeding was 3.36% per year in the warfarin group compared with 2.71% per year in the group that received dabigatran 110 mg (p=0.003) and 3.11% per year in the group that received dabigatran 150 mg (p=0.31). The rate of hemorrhagic stroke was 0.38% per year in the warfarin group compared with 0.12% per year with dabigatran 110 mg (p<0.001) and 0.10% per year with dabigatran 150 mg (p<0.001) [Connolly SJ et al. N Engl J Med 2009].
Other novel oral anticoagulants have also emerged as alternatives to VKAs for stroke prevention in AF. The Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation [ROCKET AF] found that rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolism in patients with AF. Between-group differences in the risk of major bleeding were not statistically significant. However, intracranial (0.5% vs 0.7%; p=0.02) and fatal bleeding (0.2% vs 0.5%; p=0.003) occurred less frequently in the rivaroxaban group [Patel MR et al. N Engl J Med 2011].
The Apixaban for Reduction of Stroke and Other Thromboembolism Events in Atrial Fibrillation [ARISTOTLE] trial showed that, in patients with AF, apixaban was superior to warfarin in preventing stroke or SEE (1.27% per year vs 1.60% per year; HR in the apixaban group, 0.79; 95% CI, 0.66 to 0.95; p<0.001 for noninferiority and p=0.01 for superiority), caused less bleeding (2.13% per year vs 3.09% per year; HR, 0.69; 95% CI, 0.60 to 0.80; p<0.001), and resulted in lower mortality (3.52% per year vs 3.94% per year; HR, 0.89; 95% CI, 0.80 to 0.99; p=0.047) [Granger CB et al. N Engl J Med 2011].
Each of these drugs has distinct pharmacological properties that could influence optimal use in clinical practice [Potpara TS et al. Adv Ther 2012]. Prof. Turquieh advised careful selection of patients (age) and taking advantage of 2 dosages. He also stressed the importance of renal evaluation and follow-up.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.