

Summary
Obesity is associated with a range of adverse metabolic consequences, including endothelial dysfunction, systemic inflammation, and insulin resistance. Therefore, to provide effective protection against the development of atherosclerosis and heart disease, obese patients require combination drug regimens that target several cardiometabolic risk factors.
- Obesity
- Cardiometabolic Disorder
- Hypertensive Disease
Obesity is associated with a range of adverse metabolic consequences, including endothelial dysfunction, systemic inflammation, and insulin resistance. Therefore, to provide effective protection against the development of atherosclerosis and heart disease, obese patients require combination drug regimens that target several cardiometabolic risk factors.
Kwang Kon Koh, MD, Gachon University Gil Hospital, Incheon, Korea, described the rationale for multiple targeted therapy in patients with abdominal obesity.
Adipose tissue acts as a complex endocrine organ that secretes both atherogenic cytokines, such as leptin and high-sensitivity C-reactive protein (hsCRP), and anti-atherogenic hormones, such as adiponectin. As individuals gain weight, the accumulation of visceral adipocytes leads to macrophage infiltration, increased release of atherogenic cytokines, and decreased secretion of adiponectin. Together, these pathologic mechanisms promote the development of atherosclerosis.
Moderate weight loss, defined as a loss of 5% to 10% of total body weight and 15% to 30% of visceral adipose tissue, improves cardiometabolic risk profile by lowering low-density lipoprotein (LDL) and triglyceride levels and improving glycemic control [Roberts CK et al. J Appl Physiol 2006]. However, weight loss goals are difficult to achieve. In a study of obese patients following 1 of 4 popular weight loss programs, the drop-out rate ranged from 35% to 50% after 12 months [Dansinger ML et al. JAMA 2005]. Among patients who remained in the program, the mean weight loss ranged from 4.7 to 7.1 lbs. Therefore, although moderate weight loss is an effective tool for reducing cardiometabolic risk, many obese patients will require additional interventions.
Statin-based Combination Therapy
Combination drug therapy can be tailored to address the related mechanisms that underlie obesity, diabetes, dyslipidemia, hypertension, atherosclerosis, and coronary heart disease (CHD). Statins and renin-angiotensin-aldosterone system blockers, such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), have beneficial vascular and metabolic effects in patients with multiple risk factors. For instance, in a randomized, double-blind, placebo-controlled study of 47 patients with hypertension and hypercholesterolemia, combination therapy with simvastatin 20 mg/day and losartan 100 mg/day improved vasomotor function and reduced inflammatory markers to a greater extent than statin or ARB monotherapy [Koh KK et al. Circulation 2004]. In another randomized, double-blind, placebo-controlled study of 50 patients with type 2 diabetes, combination treatment with simvastatin 20 mg/day and ramipril 10 mg/day provided a greater reduction in hsCRP levels and a greater improvement in endothelium-dependent dilation than either statin or ACE inhibitor therapy alone [Koh KK et al. Hypertension 2005].
Not all statin therapies have similar metabolic effects in patients with elevated LDL levels. Prof. Koh and colleagues showed that despite providing similar reductions and LDL levels and similar improvements in endothelium-dependent dilation, simvastatin and pravastatin had different effects on adipocytokine levels and glucose metabolism. In a study of 43 patients with hypercholesterolemia, treatment with pravastatin 40 mg/day significantly increased plasma adiponectin levels by 10% (p=0.012) and insulin sensitivity by 6% (p=0.008) compared with baseline. In contrast, treatment with simvastatin 20 mg/day significantly decreased plasma adiponectin levels by 10% (p=0.012) and insulin sensitivity by 6% (p=0.007) compared with baseline [Koh KK. Atherosclerosis 2009].
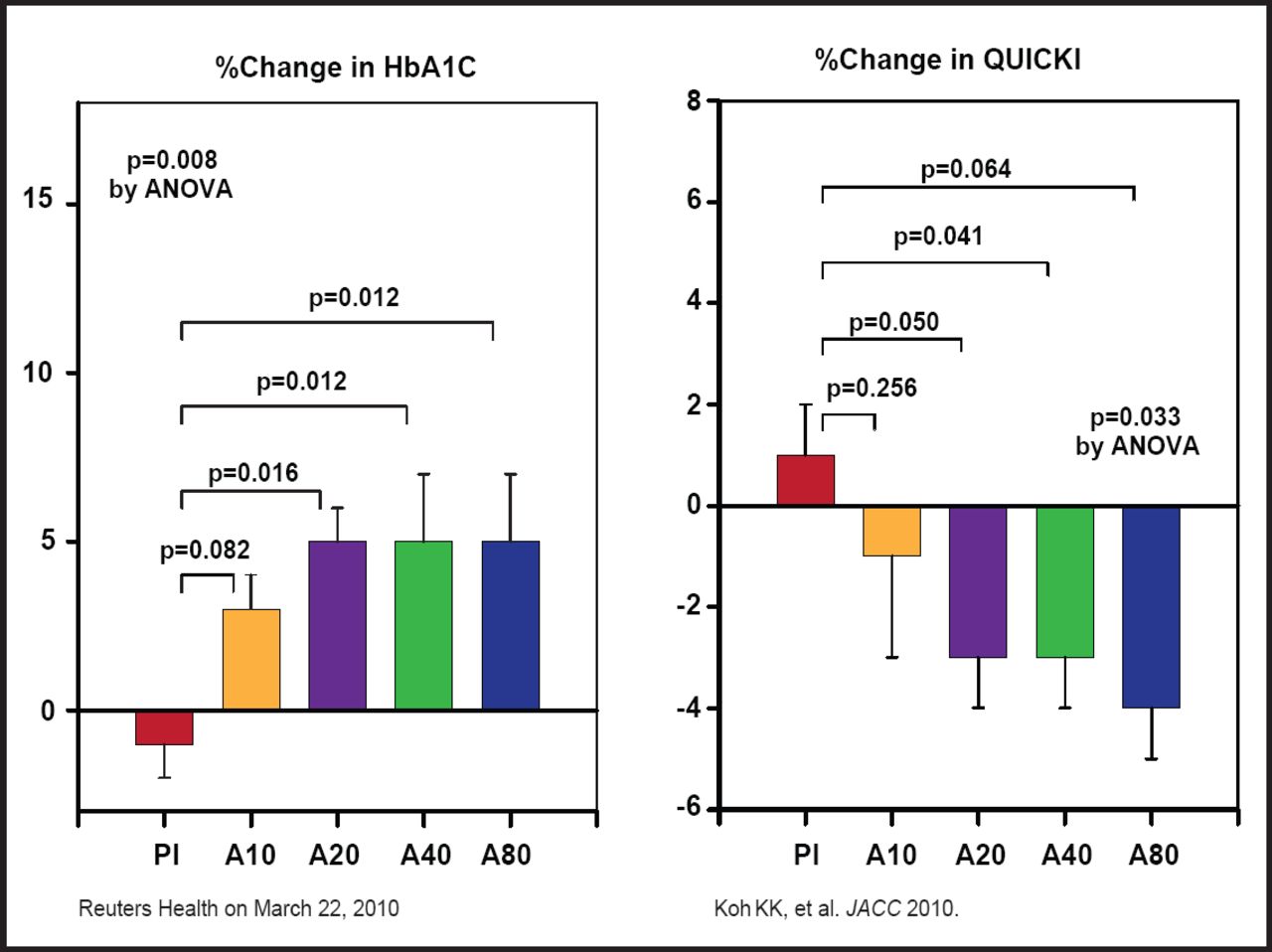
Treatment with atorvastatin also appears to adversely effect glucose metabolism. In a study of 213 patients with hypercholesterolemia, treatment with atorvastatin 10 to 80 mg/day significantly reduced LDL and apolipoprotein B levels compared with placebo after 2 months (p<0.001) [Koh KK et al. J Am Coll Cardiol 2010]. All doses of atorvastatin also significantly increased glycated hemoglobin levels (p=0.008) and significantly decreased insulin sensitivity (p=0.033) compared with placebo (Figure 1). These findings support the hypothesis that lipophilic statins, including atorvastatin, simvastatin, and rosuvastatin, might increase the onset of new diabetes in patients with hypercholesterolemia. Prof. Koh suggests a weak hydrophilic, but strong HMGCoA enzyme inhibiting statin, following rosuvastatin because rosuvastatin is not lipophilic.

Atorvastatin (10, 20, 40, or 80 mg/day) Significantly Increases HbA1C Levels and Insulin Resistance In Hypercholesterolemic Patients.
A10=atorvastatin 10 mg/day; A20=atorvastatin 20 mg/day; A40=atorvastatin 40 mg/day; A80=atorvastatin 80 mg/day; ANOVA=analysis of variance; Pl=placebo; QUICKI=Quantitative Insulin-Sensitivity Check Index.
Fibrate-Based Combination Therapy
Elevated triglyceride levels are another important target for combination therapy. According to a meta-analysis of 262,525 participants in 29 studies, there is a significant correlation between triglyceride values and CHD risk. Indeed, patients in the top tertile of triglyceride values have a 72% higher risk of CHD than those in the bottom tertile (OR, 1.72; 95% CI, 1.56 to 1.90) [Sarwar N et al. Circulation 2007].
Fibrates are emerging as an important therapeutic option for patients with elevated triglyceride levels. In addition to lowering triglyceride levels, fibrate therapy improves endothelium-dependent vasodilation, exerts anti-inflammatory effects, stabilizes atherosclerotic plaques, and inhibits platelet thrombus formation. In a meta-analysis of 18 trials, fibrates significantly reduced the risk of major cardiovascular events in patients with combined dyslipidemia (RR, 0.90; p=0.048), primarily by preventing coronary events (RR, 0.87; p<0.0001) [Jun M et al. Lancet 2010].
Fibrates also enhance the cardioprotective effects of other drug classes. In a randomized, double-blind, placebo-controlled study of 44 patients with hypertension and hypertriglyceridemia, combination therapy with fenofibrate and candesartan provided greater improvement in endothelial function and greater reduction in hsCRP level compared with fibrate or ARB monotherapy. All treatment options, including combination therapy, fenofibrate monotherapy, and candesartan monotherapy, also significantly increased adiponectin levels and insulin sensitivity compared with baseline [Koh KK et al. Diabetes Care 2006].
In summary, there are multiple etiologies for atherosclerosis and cardiovascular disease. Thus, combination therapy with drugs that have distinct and separate mechanisms of action appear to provide greater protection against cardiovascular events than individual monotherapies. Clinicians should select specific combination regimens that have been shown to provide comprehensive protection against the adverse consequences of abdominal obesity and increased cardiometabolic risk, Prof. Koh said.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.