

Summary
Type 2 diabetes mellitus (T2DM) is a progressive disease that is characterized by declining β-cell function, insulin resistance, poor glycemic control, abdominal fat accumulation, and increased risk of cardiovascular disease (CVD). Controlling obesity is particularly challenging for patients with T2DM, given that many standard T2DM medications are associated with weight gain.
- Cardiometabolic Disorder
- Diabetes Mellitus
- Hypertensive Disease
- Prevention & Screening
- Obesity
- Lipid Disorders
Type 2 diabetes mellitus (T2DM) is a progressive disease that is characterized by declining β-cell function, insulin resistance, poor glycemic control, abdominal fat accumulation, and increased risk of cardiovascular disease (CVD). Controlling obesity is particularly challenging for patients with T2DM, given that many standard T2DM medications are associated with weight gain. In the UKPDS trial, patients with T2DM gained up to 8 kg over 12 years on conventional diabetes therapy, and those in the ADOPT study gained 4.8 kg in 5 years [UKPDS Group. Lancet 1998; Kahn SE et al. New Engl J Med 2006].
Reducing the complications that are associated with abdominal obesity requires a comprehensive approach. In a session moderated by Luc Van Gaal, MD, Antwerp University Hospital, Antwerp, Belgium, presenters discussed current and emerging options for lifestyle interventions, lipid management, and blood pressure control in patients with abdominal obesity and T2DM. Presenters also discussed approaches for combining lifestyle modifications and pharmacotherapy to improve cardiometabolic risk profile.
Targeting Visceral Fat Accumulation
Michael Jensen, MD, Mayo Clinic, Rochester, Minnesota, USA
Therapeutic lifestyle interventions that are designed to promote weight loss through improved diet and increased physical activity are a critical first step toward cardiovascular risk reduction among obese patients. More specifically, an expectation of weight loss is that visceral fat volume will be reduced.
A large number of studies have explored the effects of weight loss on cardiometabolic risk profile, with consistent positive findings. Dr. Jensen described the implications of one representative study on weight management in patients with abdominal obesity. The study included 19 sedentary men and women with upper body obesity (BMI, 28–36 kg/m2) and insulin resistance. After 20 weeks of an intensive diet, behavioral therapy, and exercise intervention, the investigators observed a range of improvements in body weight, insulin sensitivity, and lipid profile (Table 1) [Shadid S et al. Diabetes Care 2003; Shadid S et al. J Clin Endocinol Metab 2006].
Effects of Diet and Exercise in Patients with Upper Body Obesity and Insulin Resistance.
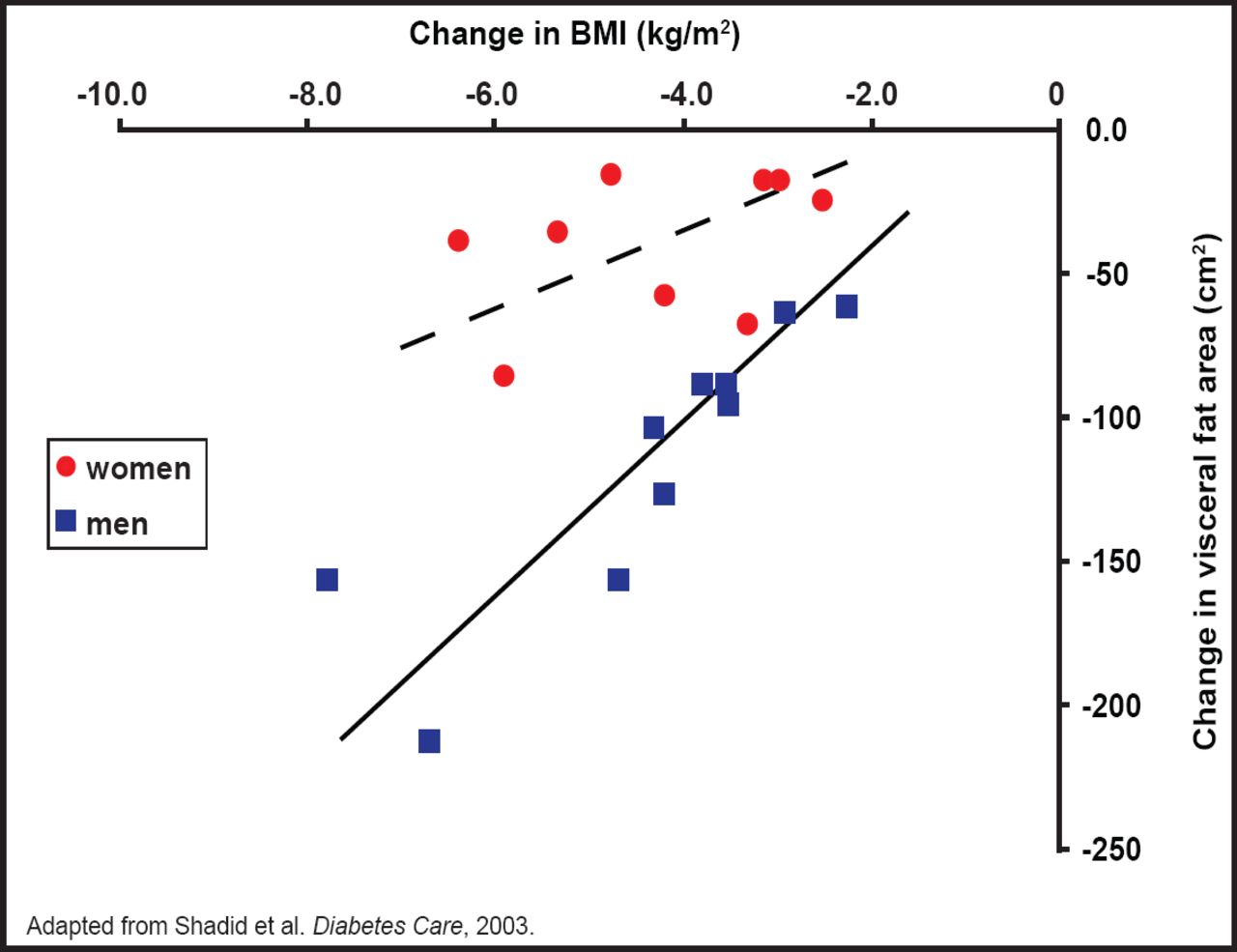
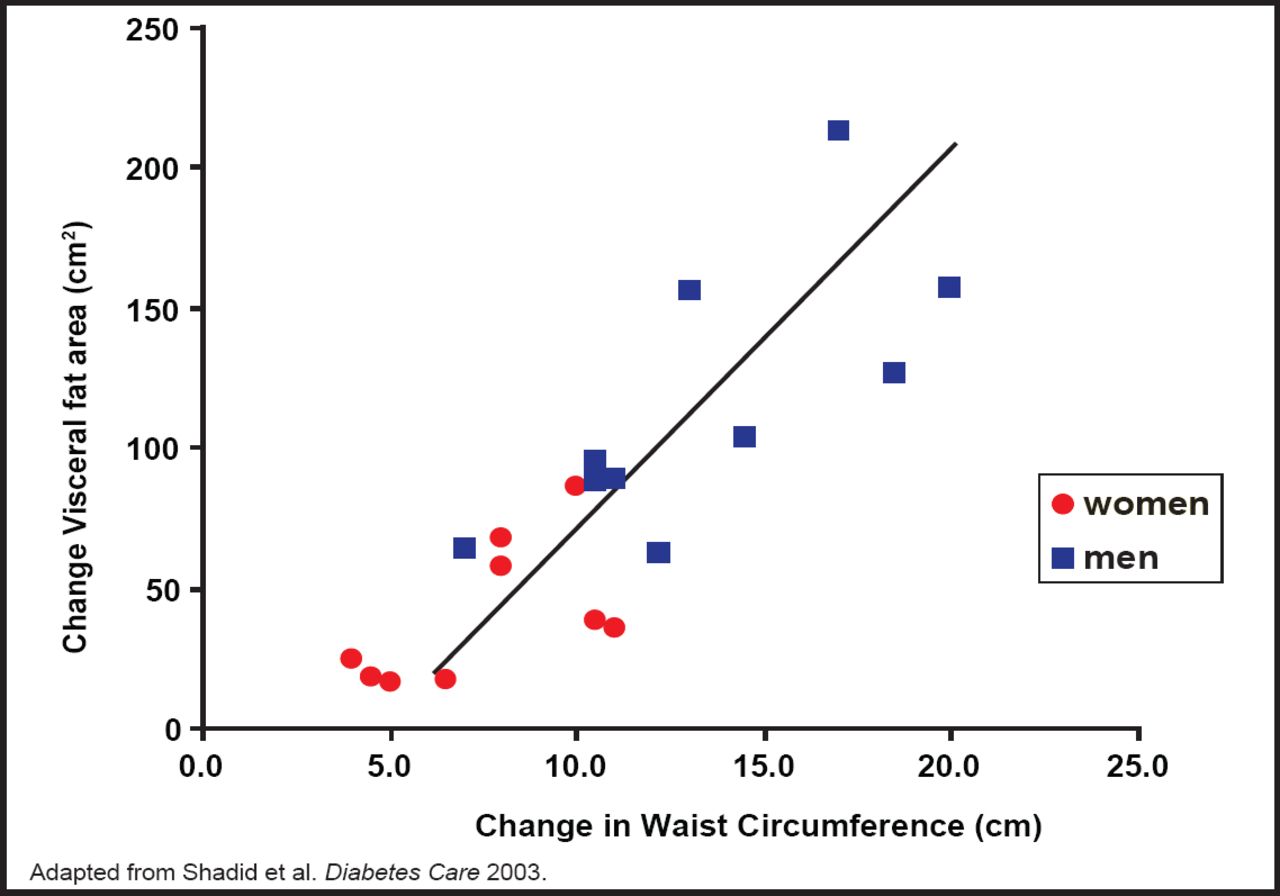
Many other published studies have confirmed these findings, although there is no complete understanding of the underlying metabolic changes that occur after weight loss yet, Dr. Jensen said. For instance, for any given decrease in BMI, men had a greater reduction in visceral fat volume than women (Figure 1). Therefore, changes in BMI must be interpreted in the context of sex-related differences in visceral fat responses. By comparison, decreases in waist circumference corresponded very well with changes in visceral fat content for both men and women (Figure 2). Thus, for both sexes, decreases in waist circumference are a clear marker of decreased visceral fat [Shadid S et al. Diabetes Care 2003; Shadid S et al. J Clin Endocinol Metab 2006].

Relationship Between Change in BMI and Change in Visceral Fat Area After Weight Loss in Men and Women.
Reproduced with permission from M. Jensen, MD.

Relationship Between Change in Waist Circumference and Change in Visceral Fat Area After Weight Loss in Men and Women.
Reproduced with permission from M. Jensen, MD.
Upper body obesity is associated with high basal and postprandial free fatty acid (FFA) concentrations. Despite the close physiological links between visceral fat, FFA, and triglycerides, the study found only a weak correlation between changes in fasting triglyceride levels and changes in visceral fat mass, as measured by CT imaging [Shadid S et al. Diabetes Care 2003; Shadid S et al. J Clin Endocinol Metab 2006].
Reduction in adipose tissue mass via negative energy balance results in improved insulin regulation of lipolysis. In this study, improved insulin sensitivity was only weakly associated with lower BMI but more strongly associated with reduced waist circumference. This reinforces the importance of reducing abdominal fat mass, not just body weight, as a predictor of improved insulin sensitivity. Improved fitness also corresponded strongly with improved insulin sensitivity, highlighting the role of exercise-induced increases in muscle insulin sensitivity in improving overall cardiometabolic profile.
Together, these findings demonstrate the benefits of visceral fat loss on glucose metabolism and lipid profile in obese patients with insulin resistance. Therapeutic interventions should emphasize the importance of abdominal fat loss, which is monitored easily in the clinical setting by measuring waist circumference.
Targeting Dyslipidemia
H. Bryan Brewer, Jr., MD, MedStar Research Institute, Washington, DC, USA
Lipid-lowering therapy reduces the risk of major vascular events in patients with T2DM and dyslipidemia. In the Heart Protection Study, treatment with simvastatin was similarly effective in patients with diabetes and without diabetes in lowering the risk of stroke, revascularization, major vascular events, and major coronary events by approximately 25% versus placebo [MRC/BHF Heart Protection Study Group. Lancet].
Despite the proven cardioprotective benefits of lipid-lowering therapy, patients who are treated with statins still have significant residual cardiovascular risk. To improve cardiovascular outcomes, lipid-modifying therapy must target additional risk factors, such as high-density lipoprotein (HDL). In a study of patients with acute coronary syndrome (ACS), low HDL was an independent risk factor for increased cardiac events and mortality. Regardless of baseline low-density lipoprotein (LDL) levels and statin use, patients with low HDL (<40 mg/dL in men and <45 mg/dL in women) had a 3-fold higher risk of cardiac events and death after 1 year (HR, 3.33; 95% CI, 1.15 to 10.0) [Wolfram RM et al. Am J Cardiol 2006].
Targeting HDL may be particularly important for patients with T2DM, who have dysfunctional HDL metabolism. In healthy persons, HDL provides a range of cardioprotective effects on the vascular endothelium, including increased endothelial nitric oxide production, reduced endothelial oxidant stress, improved endothelium-dependent vasodilation, and early endothelial repair. By comparison, the endothelial-protective effects of HDL in patients with T2DM are substantially impaired [Sorrentino SA. Circulation 2010].
Current options for HDL-targeted therapy in patients with abdominal obesity and T2DM include fibrates, combination fibrate/statin therapy, and niacin. Combination treatment with fenofibric acid and statin therapy provides a greater increase in HDL than either agent used as monotherapy. In a Phase III trial in patients with mixed dyslipidemia, mean HDL increased by 16.2 mg/dL in the ABT-335 group, 7.2 mg/dL in the simvastatin group, and 17.8 mg/dL in the ABT-335/simvastatin combination group (p<0.001 vs simvastatin monotherapy) after 12 weeks [Mohiuddin SM et al. Am Heart J 2009].
Treatment with extended-release (ER) niacin therapy provides a significantly greater improvement in HDL plasma levels than placebo in patients with T2DM and metabolic syndrome (+6.0 mg/dL vs −2.0 mg/dL; p<0.001). In these patients, ER niacin also improves endothelial-protective functions of HDL, which is important for improving cardiometabolic risk profile [Sorrentino SA. Circulation 2010].
Targeting Hypertension
Paul Poirier, MD, Quebec Heart and Lung Institute, Quebec, Canada
For patients with T2DM, keeping systolic blood pressure (SBP) within the recommended target range (130 mm Hg to 135 mm Hg or lower) involves the use of combination antihypertensive medications and aggressive lifestyle interventions. The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial recently compared different hypertension management strategies in 4733 patients with T2DM [ACCORD Study Group. New Engl J Med 2010]. Patients were randomly assigned to an intensive strategy that targeted SBP <120 mm Hg or to standard therapy that targeted SBP <140 mm Hg. After 1 year, patients in the intensive and standard therapy groups achieved mean SBP levels of 119.3 mm Hg and 133.5 mm Hg, respectively. Reaching these blood pressure goals required an average of 3.4 antihypertensive medications in the intensive group and 2.3 medications in the standard treatment group.
After 4.7 years, patients in both treatment groups were equally likely to reach the primary outcome of nonfatal myocardial infarction (MI), nonfatal stroke, or death from CVD (HR, 0.88; p=0.20). However, patients in the intensive group had a lower risk of nonfatal stroke (HR, 0.63; p=0.03) and total stroke (HR, 0.59; p=0.01). Overall, findings from the ACCORD trial suggest that intensive blood pressure control provides no additional protection against total cardiovascular events relative to standard antihypertensive therapy but may reduce the risk of stroke [ACCORD Study Group. New Engl J Med 2010].
Current hypertension guidelines recommend intense nonpharmacological interventions in all patients with T2DM, with particular attention to weight loss and reduction of salt intake [Mancia G et al. J Hypertens 2007]. In a meta-analysis of hypertensive trials, weight loss correlated strongly with significant improvements in SBP and diastolic blood pressure (DBP) [Horvath K et al. Arch Intern Med 2008]. In the Look AHEAD (Action of Health in Diabetes) trial, intensive lifestyle modification was better than standard diabetes education and support in improving fitness (p<0.001), promoting weight loss (p<0.001), and decreasing SBP (p<0.001) and DBP (p=0.01) [Look AHEAD Research Group. Arch Intern Med 2010].
To successfully manage hypertensive patients, clinicians should identify potential barriers to treatment adherence and long-term weight loss. By developing individualized treatment approaches, clinicians can help patients achieve and maintain their blood pressure and weight loss goals.
Combining Lifestyle Interventions and Drug Therapy
Darren McGuire, MD, University of Texas Southwestern Medical Center, Dallas, Texas, USA
The prevalence of T2DM is increasing, especially among patients with established CVD. For many, the principal risk that is associated with T2DM is atherosclerotic vascular disease. Therefore, it is important to expand the focus of diabetes management from glycemic control to global cardiovascular risk reduction.
All patients with T2DM should be managed with lifestyle interventions that are aimed to decrease body weight, increase physical activity, and maintain target blood pressure levels (<130/80 mm Hg). Therapeutic lifestyle interventions can rapidly and dramatically improve cardiovascular risk profile. In a community-based study of 2390 patients with hypertension, hyperlipidemia, and/or impaired fasting glucose or T2DM, therapeutic lifestyle changes reduced SBP by 17 mm Hg, DBP by 10 mm Hg, LDL by 0.2 mmol/l, and fasting glucose by 1.0 mmol/l in 12 weeks (p<0.05 vs baseline for all measures) [Gordon NF et al. Am J Cardiol 2004].
First-line pharmacotherapy is appropriate for all adults aged 40 years or older with at least one cardiovascular risk factor and for all persons with established CVD [Diabetes Care]. Treatment should include daily statin therapy, dosed to achieve LDL goals of <2.6 mmol/l (<100 mg/dL). An optional LDL goal of <1.8 mmol/l (<70 mg/dL) is appropriate for high-risk individuals. Aggressive blood pressure control with a combination of therapeutic lifestyle changes, sodium restriction, and pharmacotherapy should be a focus of therapy, with a target of therapy to achieve BP <130/80. For men aged >55 years and women aged >60 years who have concomitant cardiovascular risk factors or younger patients with prevalent CVD, treatment should include aspirin (75–162 mg daily), especially for those who have already had a cardiovascular event. For persons aged 55 years or older with any cardiovascular risk factor or for any patient with CVD, add-on therapy with an ACE inhibitor should also be considered independently of blood pressure targets.
In the Steno-2 study, intensive intervention with multiple drug combinations and lifestyle modification that is targeted at global cardiovascular risk reduction significantly reduced cardiovascular morbidity and mortality compared with standard care in patients with T2DM. Patients in the intensive therapy group were managed with the following treatment goals: HbA1C <6.5%, total cholesterol <4.5 mmol/l (175 mg/dL), triglycerides <3.9 mmol/l (150 mg/dL), and blood pressure <130/80 mm Hg. After 13.3 years of follow-up, patients in the intensive therapy group had a 59% lower risk of cardiovascular events (HR, 0.41; p<0.001) and a 47% lower risk of cardiovascular death (HR, 0.43; p=0.04) compared with those in the conventional therapy group [Gaede P et al. New Engl J Med 2008].
In summary, therapeutic lifestyle changes are an important first step toward cardiovascular risk reduction for all patients. Combination pharmacotherapy with aspirin, a statin, and an ACE inhibitor provides additional protection against cardiovascular events.
Abdominal Obesity and Heart Surgery
Patrick Mathieu, MD, Université Laval, Québec, Canada
Visceral obesity can lead to several potential complications that require surgical intervention. For instance, abdominal fat accumulation is associated with structural valve deterioration (SVD) and aortic valve disease. Aortic calcification is a highly prevalent condition, especially among elderly patients. Up to 25% of individuals aged 65 years and older have aortic stenosis (AS), which results from progressive calcification of aortic tissues. Over time, AS leads to left ventricular hypertrophy (LVH) and symptoms such as dyspnea, angina, heart failure, and sudden cardiac death.
The pathological mechanisms that underlie calcific AS are similar to those of atherosclerosis, including the vascular infiltration of oxidized LDL and inflammatory cells. Moreover, the atherogenic and inflammatory abnormalities that are associated with abdominal obesity and metabolic syndrome appear to accelerate the progression of AS. In the Multi-Ethnic Study of Atherosclerosis (MESA), diabetes and metabolic syndrome were associated with a higher prevalence of aortic valve calcification [Katz R et al. Circulation 2006]. In another study of patients with severe AS who were undergoing an aortic valve replacement, a greater proportion of small, dense LDL particles in the plasma was associated with faster progression of valvular stenosis and greater accumulation of oxidized LDL in the aortic valve [Mohty D et al. Thromb Vasc Biol 2008].
Abdominal obesity is also a risk factor for poor outcomes, including postoperative atrial fibrillation and mortality, in patients who are undergoing cardiac surgery. In a study of 5304 patients who were undergoing coronary artery bypass grafting, 43% of patients had metabolic syndrome. The presence of metabolic syndrome increased the risk of in-hospital mortality more than 3-fold (HR, 3.04; 95% CI, 1.73 to 5.32; p=0.0001) [Echahidi N et al. J Am Coll Cardiol 2007].
In summary, visceral obesity is an important cardiovascular risk factor that accelerates the development of cardiac disorders and adversely affects the surgical outcomes of affected individuals. Decreasing the prevalence of visceral obesity may reduce the burden of aortic valve disease and improve the prognosis for patients with CVD. Pharmacological interventions that target small, dense LDL particles may also disrupt the link between visceral obesity and AS.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.