

Summary
The role of low-dose aspirin as primary prevention among individuals who are at high risk for cardiovascular disease is controversial. Given the greater risk for cardiovascular events among individuals with diabetes, antiplatelet therapy has appeal as a way to reduce the risk of thrombi and subsequent ischemic events in both the primary and secondary setting.
- Prevention & Screening
- Thrombotic Disorders
- Diabetes Mellitus
- Myocardial Infarction
The role of low-dose aspirin as primary prevention among individuals who are at high risk for cardiovascular disease (CVD) is controversial. Given the greater risk for cardiovascular (CV) events among individuals with diabetes, antiplatelet therapy has appeal as a way to reduce the risk of thrombi and subsequent ischemic events in both the primary and secondary setting.
Aspirin for Primary Prevention
The great interest—and uncertainty—about the role of aspirin as primary prevention has been demonstrated by the number of recent meta-analyses on aspirin trials, said Nilay Shah, MD, Mayo Clinic, Rochester, Minnesota, USA. In the most recent meta-analysis, aspirin decreased the risk for CV events and nonfatal myocardial infarction (MI), but there were no significant differences in the incidence of stroke, CV or all-cause mortality, or total coronary heart disease [Bartolucci AA et al. Am J Caridiol 2011]. Five other meta-analyses that focused on patients with diabetes demonstrated a nonsignificant reduction in CV events (Table 1).
Summary of Evidence.
Despite the benefits that are associated with aspirin, the benefits must be weighed against the risk of excess bleeding. “Heterogeneity exists in the risk-benefit tradeoff of aspirin,” said Dr. Shah, increasing the challenge of decision-making.
Most of the benefit of aspirin for men is derived from a reduction in MIs, whereas the greatest benefit for women is a reduction in strokes [Berger JS et al. JAMA 2006]. This difference in benefit is reflected in the United States Prevention Services Task Force guideline, which recommends aspirin for primary prevention for men aged 45 to 79 years and women aged 55 to 79 years when the CV risk outweighs harm; specific risks are defined for each gender and age group (Table 2) [Wolff T et al. Ann Intern Med 2009]. There is no differentiation in recommendations for individuals with diabetes.
Definitions of Risk in the US Preventive Services Task Force Recommendations for Aspirin as Primary Prevention.
The guidelines that were set forth by the American Diabetes Association (ADA)/American Heart Association (AHA)/American College of Cardiology Foundation (ACCF) in 2010 “are quite different than the 2002 guidelines,” said Dr. Shah. The new guideline notes that aspirin therapy for primary prevention may be considered for individuals with type 1 or type 2 diabetes who are at increased CV risk, which is defined as a 10-year risk >10%. The guideline does not recommend aspirin for individuals with diabetes and a low CV risk (10-year risk <5%) and notes that clinical judgment is required for individuals with a 10-year CV risk of 5% to 10% [Pignone M et al. Diabetes Care 2010]. There is no differentiation according to gender.
These risk thresholds raise several issues. At the population level, if the guideline thresholds are used, an estimated 54 million individuals who take preventive aspirin would benefit, with most of the benefit found among people with a 10-year risk >20% and little benefit found for individuals with a 6% to 10% risk [Sussman JB et al. Circ Cardiovasc Qual Outcomes 2011]. Among the diabetes population, the greatest proportion of individuals (53%) has a CV risk of 10% to 20%, and approximately one-third has a risk >20%.
The issue of risk is further complicated by the use of additional treatments, as people who are at high CV risk typically take antihypertensives and statins to reduce their risk. The unanswered question of the incremental benefit of aspirin adds complexity to the decision-making process about aspirin use.
Patients with diabetes already face many challenges, with high numbers of diabetes-related medications, comorbidities, and health care visits. He encouraged clinicians to find ways to engage their patients in making an informed choice about aspirin use. Patients' preferences and how they value the risk-benefit ratio of aspirin are integral to the decision-making process about aspirin for primary prevention.
Role of Intensive Platelet Therapy
Can the benefit of aspirin as primary prevention be improved with the addition of another antiplatelet drug? “There is no evidence for improved efficacy beyond aspirin,” said Stephen D. Wiviott, MD, Cardiovascular Division, Brigham and Women's Hospital, Boston, Massachusetts, USA. He pointed to the results of the CHARISMA trial, in which low-dose aspirin plus clopidogrel was not more effective than aspirin alone in reducing the rate of MI, stroke, or CV deaths among participants who had either stable CVD or multiple CV risk factors (including type 1 and type 2 diabetes) [Bhatt DL et al. NEJM 2006]. In the group of subjects with multiple risk factors, there was a trend that favored aspirin alone, with increased bleeding and higher mortality rates associated with dual antiplatelet therapy.
Although intensive therapy may not be beneficial as primary prevention, “the net benefit may be greater in patients with ACS [acute coronary syndrome] and diabetes,” said Dr. Wiviott. “Patients with diabetes have higher event rates with similar or greater reductions in ischemic events with intensive platelet therapy,” he added, discussing the findings of several landmark trials to support the statement.
For example, a pooled analysis of data on patients with ACS showed significantly higher all-cause mortality through 1 year after ACS for patients with diabetes compared with patients without diabetes [Donahoe SM et al. JAMA 2007]. Rates of stent thrombosis have also been substantially higher among patients with diabetes, with rates 2 to 3 times higher than those among patients without diabetes [Kuchulakanti PK et al. Circulation 2006]. Dr. Wiviott emphasized the importance of this finding, noting that stent thrombosis is the “most dreaded complication” of percutaneous coronary interventions (PCIs) and is associated with higher mortality among all groups of patients.
Intensive antiplatelet therapy has been shown to reduce the risk of these events among all patients (with and without diabetes). For example, in the CURE trial, when compared with aspirin plus placebo, aspirin plus clopidogrel was associated with lower rates of CV death/MI/stroke after many types of intervention—medical therapy alone, PCI, or coronary artery bypass grafting [Fox KA et al. Circulation 2004]. When the results were compared for patients with and without diabetes, the number of CV events was higher in both treatment groups.
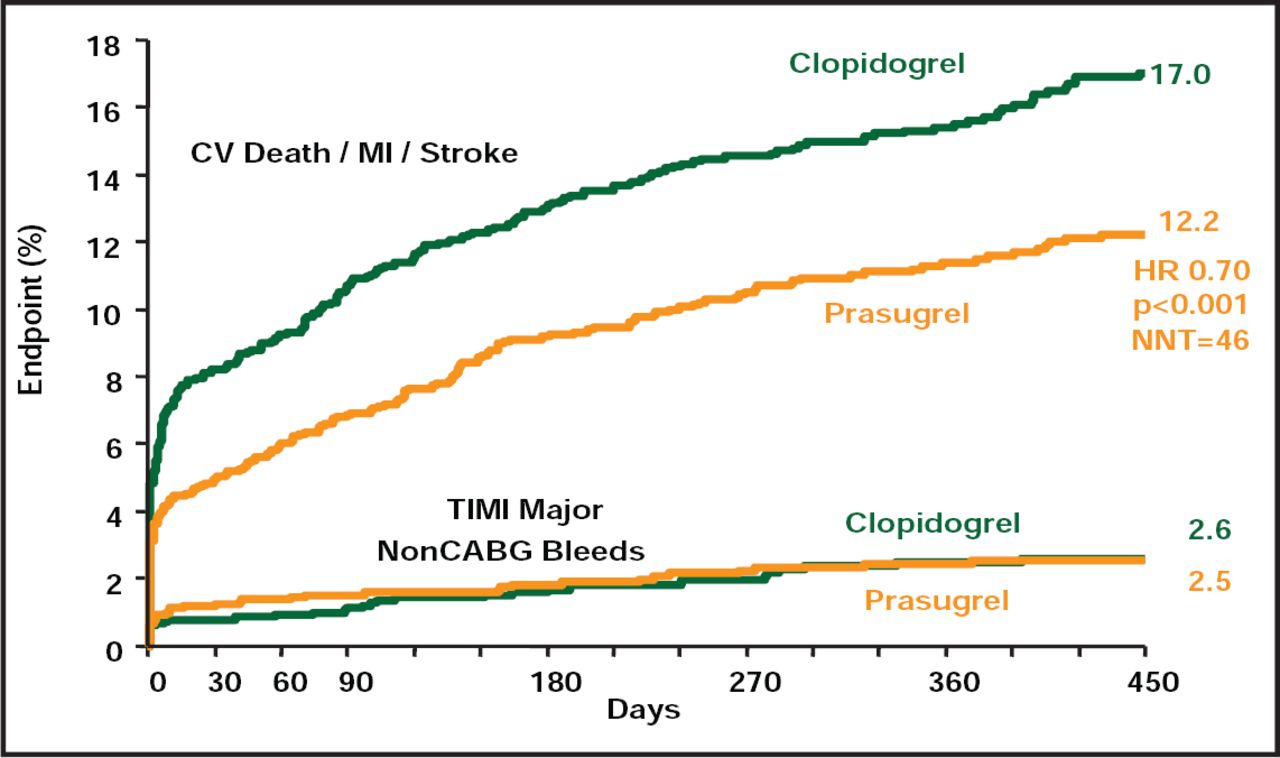
Because of the great variability in response to clopidogrel, other, more potent thienopyridines have been developed and compared with clopidogrel. One of these newer agents, prasugrel, was compared with clopidogrel in the TRITON-TIMI 38 trial, which enrolled patients with ACS and a scheduled PCI. Prasugrel was associated with significantly lower rates of CV death/MI/stroke (p<0.001) but an increase in major bleeding (p=0.03) [Wiviott SD et al. NEJM 2007]. Again, when the data for patients with and without diabetes were compared, the event rate was higher and the benefit was greater in the diabetic subgroup, with an absolute benefit of 5% (Figure 1) [Wiviott SD et al. Circulation 2008]. There was no increase in bleeding events, granting a greater net benefit to prasugrel.

TRITON-TIMI 38 Trial: Diabetic Subgroup.
Reproduced with permission from Wolters Kluwer Health; Greater Clinical Benefit of More Intensive Oral Antiplatelet Therapy With Prasugrel in Patients With Diabetes Mellitus in the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel-Thrombolysis in Myocardial Infarction 38; Wiviott SD et al. Circulation 2008;118:1626–1636.
When another agent, ticagrelor, was compared with clopidogrel among patients with ACS in the PLATO trial, ticagrelor significantly lowered rates of MI (p=0.005) and death from vascular causes (p=0.001) [Wallentin L et al. NEJM 2009]. Subsequent analysis indicated that ticagrelor was superior to clopidogrel in reducing CV events among the subgroup of patients with diabetes (14.1% vs 16.2%) [Ferreiro JL et al. Circulation in press].
Ongoing trials, such as the ASCEND (NCT00135226) and ACCEPT-D (ISRCTN48110081) trials, will help to better define the benefit of aspirin as primary prevention, specifically among patients with diabetes. In addition, researchers are continuing to explore alternate pathways of platelet inhibition to develop potent antiplatelet drugs with minimal risk of bleeding.

The editors would like to thank the many members of the American Diabetes Association 71st Scientific Sessions presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.