

Summary
This article discusses a stepwise practical guide to managing stent thrombosis, which is multifactorial, involving issues that are related to the patient, lesion, device, procedure, platelet and coagulation factors, and stent-artery interactions.
- thrombotic disorders
- interventional techniques & devices
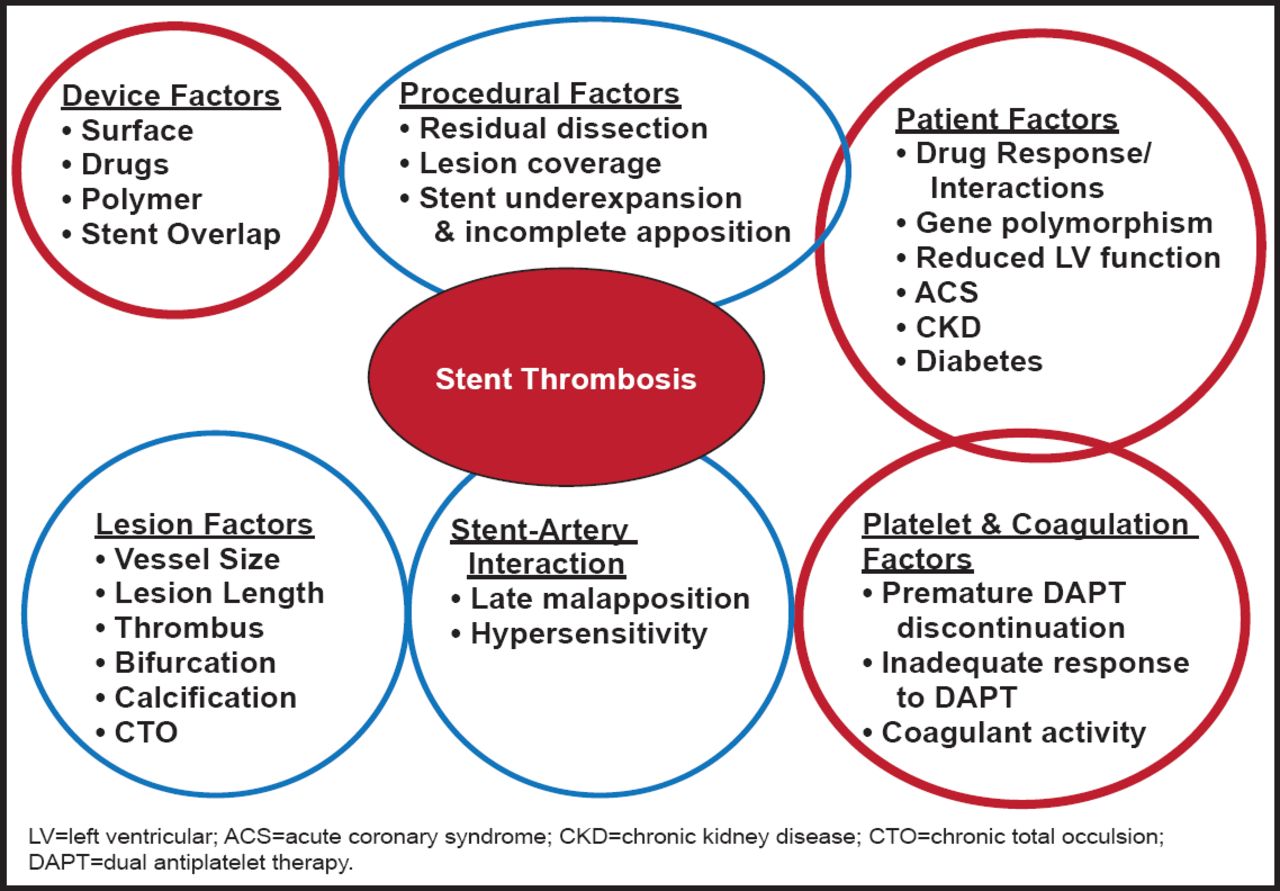
The etiology of stent thrombosis is multifactorial, involving issues that are related to the patient, lesion, device, procedure, platelet and coagulation factors, and stentartery interactions (Figure 1). Stent thrombosis is associated with a high mortality rate and needs to be recognized and diagnosed promptly. Hany Eteiba, MD, Glasgow Royal Infirmary, Glasgow, Scotland, discussed a stepwise practical guide to managing this challenging condition.

Multifactorial Nature of Stent Thrombosis.
Reproduced with permission from H. Eteiba, MD.
It is well documented that stent thrombosis can occur long (>1 year) after stent implantation and that it occurs equally with bare mental (BMS) and drug-eluting (DES) stents. Often, there is an association with interruption in dual antiplatelet therapy (DAPT). The clinical outcome following stent thrombosis is poor for patients with either BMS or DES [Burzotta F et al. Eur Heart J 2008]. In one study, after 2 years, the recurrence rate for stent thrombosis with DES was in excess of 5% and the mortality rate was ∼20%, regardless of whether the thrombosis occurred early (<30 days), late (31 to 365 days), or very late (>1 year) after stent implantation [Kimura T et al. Circulation 2010].
Proper management of stent thrombosis begins with a correct diagnosis. Since stent thrombosis usually presents with ST-segment elevation myocardial infarction, the possibility should be considered, even if it has been many years since stent implantation and even in the case of a BMS. In particular, there should be a high level of suspicion following cessation of DAPT [Airoldi F et al. Circulation 2007]. Since it is likely that a high thrombotic burden is caused by this event, rapid initiation of adjunctive pharmacotherapy with intravenous antiplatelet agents (eg, glycoprotein IIb/IIIa antagonists) and/or oral antiplatelet therapy (eg, prasugrel, ticagrelor) should be considered. Anticoagulation with weight-adjusted unfractionated heparin can be used, although bivalirudin is a reasonable alternative that is associated with less bleeding than heparin.
Rapid and careful diagnostic angiography should be considered. Radial access may make sense in centers with experience, bearing in mind that since the thrombus often propagates proximally, it will be difficult to see much in the distal vessel. It is also important to consider that there might be new disease that is adjacent to the stent, particularly in early stent thrombosis. ‘Stent boost’ technology, a new technique that improves fluoroscopy-based assessment of stent expansion, may also be useful for more slender patients. The next step is wiring, with consideration for whether rewiring or a support wire is needed. Thrombectomy should be attempted before any other instrumentation. A smaller catheter with stylet (eg, Pronto LP) is often easier and can also be used to administer adenosine or intracoronary GP IIb/IIIa antagonists if there is slow/no reflow. Intravascular ultrasound (IVUS) is strongly recommended at this point to assess the intraluminal anatomy. Optical coherence tomography imaging is more sensitive than IVUS and can provide even more information, such as the extent of new intimal coverage. Reintervention depends on the cause of the stent thrombosis. In the case of stent strut malapposition, an appropriate intervention is IVUS-guided noncompliant balloon to high-pressure angioplasty, whereas if there is no mechanical problem or malapposition and the problem is inappropriate DAPT cessation, it may be sufficient to do plain balloon angioplasty with high-pressure semicompliant balloon to ensure that the stent is wide open. It may not be necessary to do more than pharmacological thrombectomy. Restenting should be avoided when possible, as it has been associated with worse outcomes [Burzotta F et al. Eur Heart J 2008]. Slow flow is an independent predictor of poor outcome, and use of glycoprotein IIa/IIIb to improve flow should be considered. Finally, post-reintervention management is dependent on the cause of the thrombosis; however, other factors that should be considered include platelet function testing (eg, VerifyNow) and the use of newer ADP receptor blockers (eg, prasugrel/ticagrelor) for 1 year as well as patient education, particularly if compliance is an issue.
In the management of stent thrombosis, early and accurate diagnosis is critical and should be followed by appropriate pharmacology and intervention. IVUS is vital for a good reintervention. Restenting should be avoided if possible, and careful thought should be given to appropriate antiplatelet therapy and patient education.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.