

Summary
This article discusses progress in the development of a West Indies Cardiac Surgery Database.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
Randolph Rawlins, MBBS, FRCS (Ed), FRCS (C/TH), the Doctor's Inn Research Group (DIRG), Trinidad and Tobago, West Indies, discussed progress in the development of a West Indies Cardiac Surgery Database.
According to Mr. Rawlins, cardiac surgery is the first discipline to establish a major international registry of patient characteristics and outcomes. He noted that national registries of adult cardiac surgery have already been established in European countries, the United States, Canada, and elsewhere. “The UK Cardiac Surgical Register dates back to 1977,” he said.
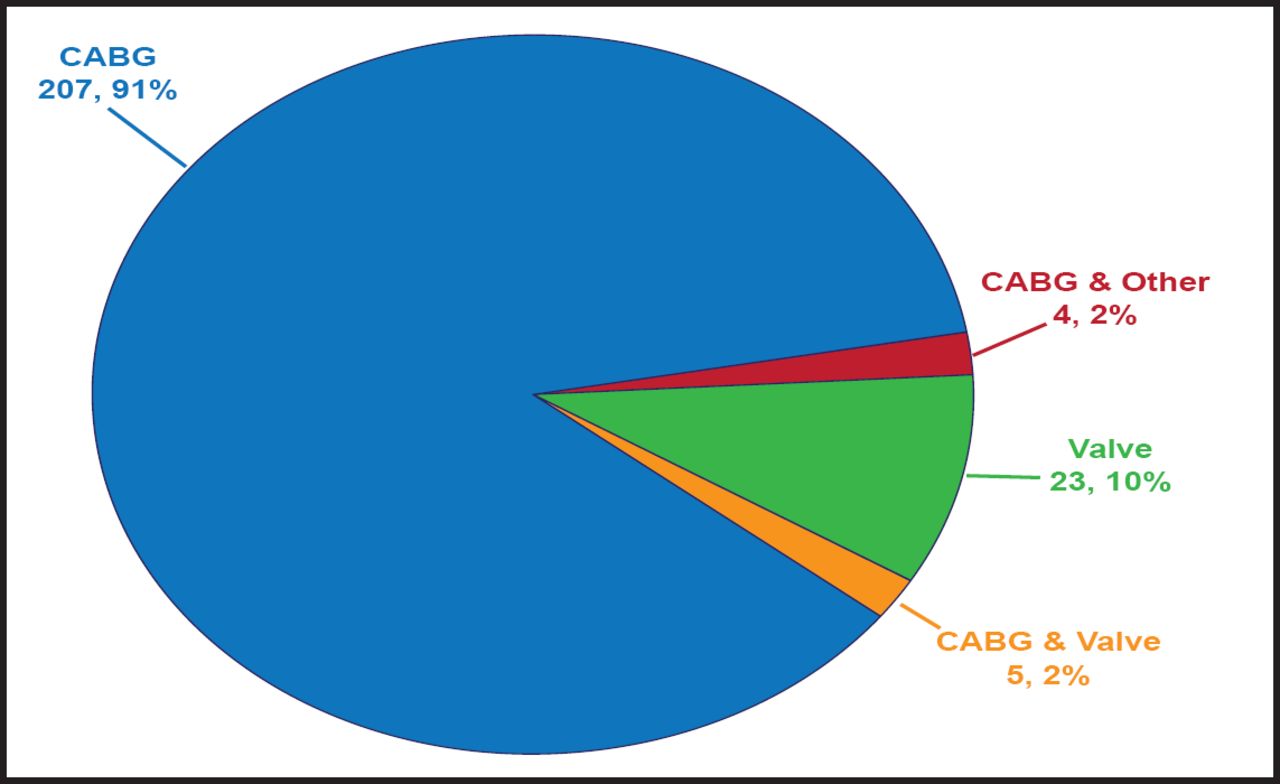
In the West Indies, 207 coronary artery bypass grafts (CABGs) accounted for 91% of all cardiac surgeries. Other operations included 23 (10%) valve, 4 (2%) CABG only, and 5 (2%) combined CABG and valve surgeries (Figure 1). Of these patients, 17% was aged <50 years; 35% was aged 50 to 59 years; 31%, 60 to 69 years; 15%, 70 to 79 years; and 3%, 80 to 90 years. The in-hospital mortality rate was 5 patients out of 227.
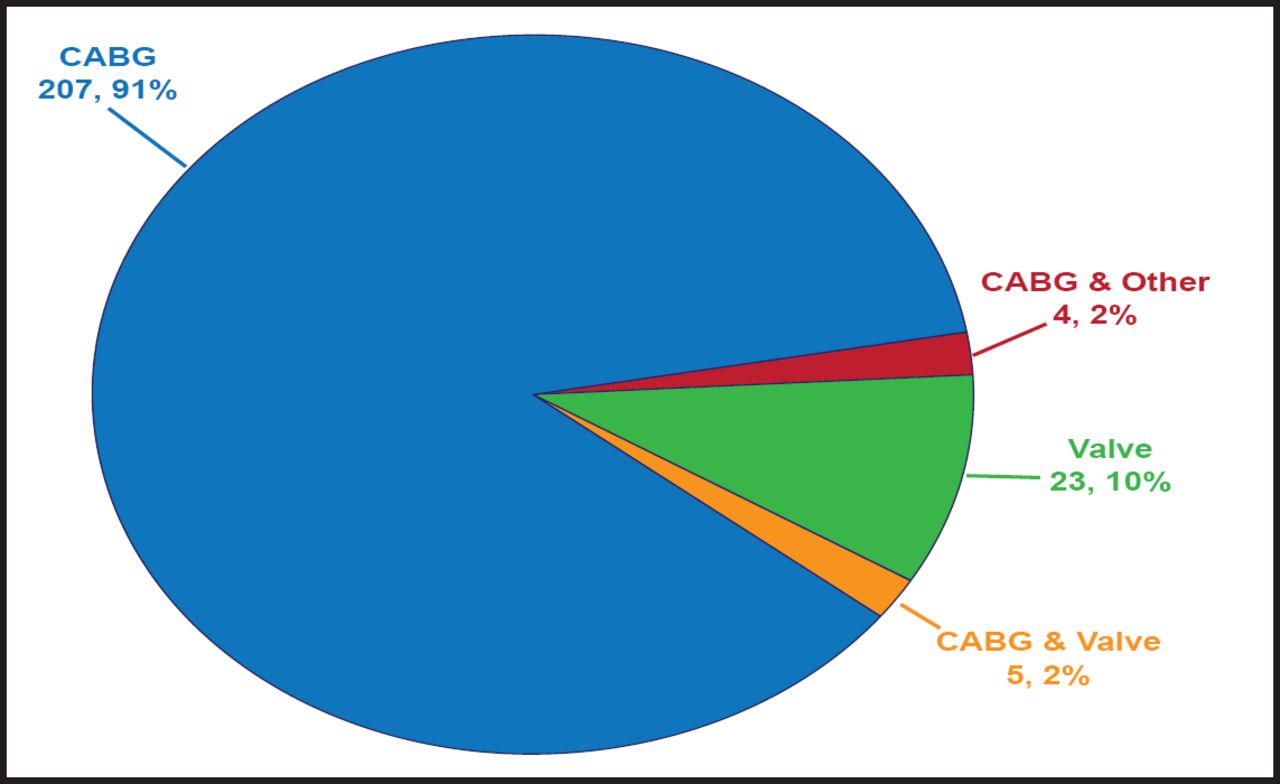
Types of Cardiac Surgery in the West Indies.
Reproduced with permission from R. Rawlins, MBBS.
Data from local units and hospitals can be important for surgeons and surgical units, in that it can be used to create locally relevant risk models. However, data from other national registries can be useful to compare outcomes in one's own country with international benchmarks. “A risk-adjusted database can help surgeons advise their patients on the chances of a good operative outcome,” he said.
To date, funding for the West Indies Cardiac Surgical Database has come from various sources, including Ministries of Health, participating surgical centers, and surgical software vendors. Industries in Trinidad and Tobago have also promised support for a database project.
DIRG has proposed a list of 55 variables to the Caribbean Cardiac Society for a pilot project. They run the gamut from demographics to intraoperative, patient-, and cardiac-related factors—eg, left ventricular function, active endocarditis, tricuspid valve, recent myocardial infarction, and unstable angina.
Issues that were identified by Mr. Rawlins included the need for dedicated resources in each hospital for data collection and collation, including IT infrastructure and “database managers.” Ideally, the dataset should be centrally defined, with local teams empowered to collect information in ways that best suit their hospitals. The dataset should not be too extensive or be changed frequently. In addition, he noted the importance of compliance with data protection legislation and patient confidentiality principles and the key roles that are played by clinical leaders.
Other issues to bear in mind during registry development include the need to involve all cardiac centers and to recognize that in the early stages, the quality of the data may be limited. He pointed out that the initial effort does not have to be perfect before data is collected and used and that the final stimulus to complete data collection is publication of surgical results.
According to Mr. Rawlins, establishing a Prospective West Indies Cardiac Surgical Database should be a priority. Information from this resource would be of value to surgeons, cardiologists, and other health care professionals, and the registry would advance research, training, and professional development.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.