

Summary
This article discusses the contribution of registries to advancements in the treatment of cardiovascular disease.
- Prevention & Screening Clinical Trials
“The only way to learn more about cardiovascular disease is to document what we know, follow patients with multiple risk factors to see if we can identify new risks for cardiovascular disease (CVD), and monitor patients after treatment so we can develop new therapies,” said Gregory R. Giugliano, MD, Baystate Medical Center, Springfield, Massachusetts, USA, who discussed the contribution of registries to advancements in the treatment of CVD.
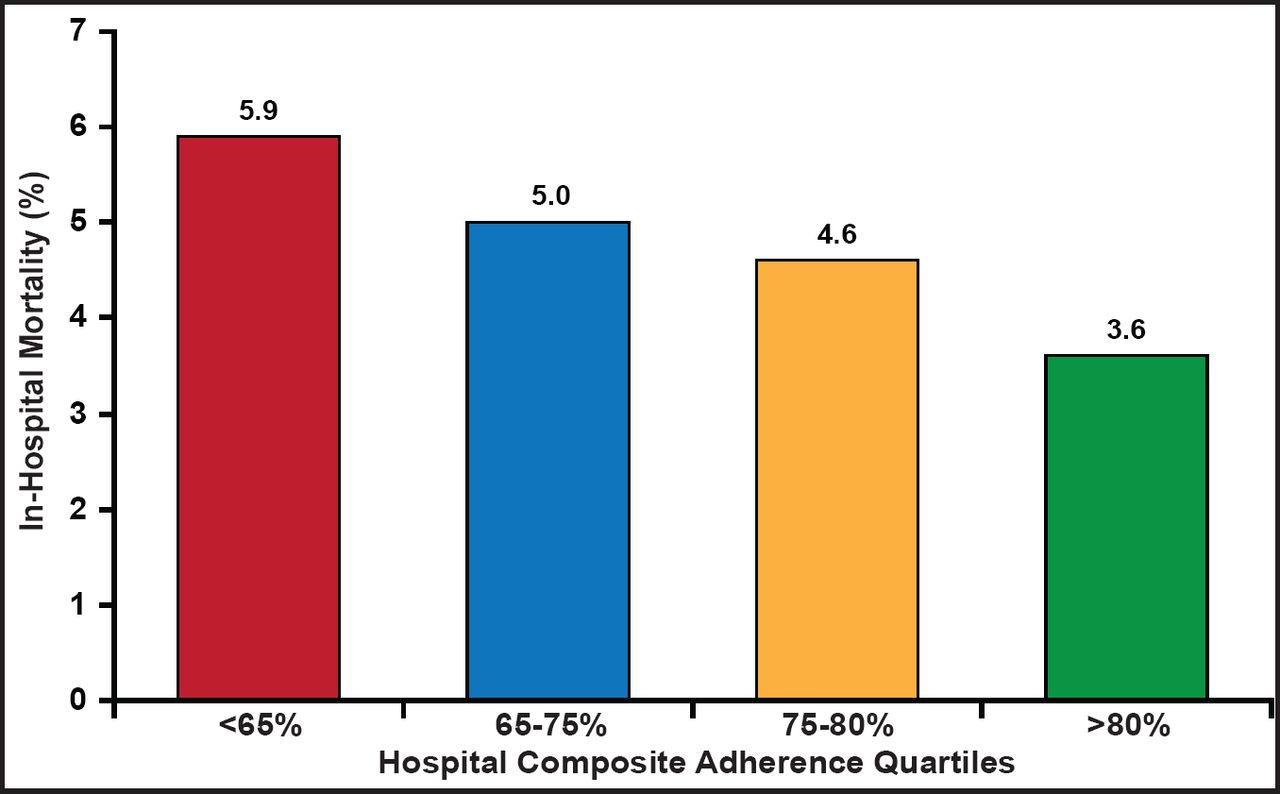
The CRUSADE Registry was a an American quality improvement (QI) initiative that involved a collaborative, multidisciplinary effort with contributions from emergency medicine, cardiology, hospital QI, academia, and industry. The purpose of the registry was to optimize the understanding and risk stratification of acute coronary syndrome (ACS) patients; evaluate adherence to American College of Cardiology/American Heart Association (ACC/AHA) treatment guidelines; and implement QI interventions through regional educational meetings, site surveys, provision of educational and QI materials, and quarterly feedback reports. The success of the QI initiative was measured by changes in adherence to the AHA/ACC treatment guidelines. Data were collected between July 2001 and December 2006 from over 500 sites (25% academic; 68% with percutaneous coronary intervention/coronary artery bypass graft [PCI/CABG]). More than 200,000 data collection forms were received (190,000 non-ST elevation myocardial infarction (NSTEMI); 8800 STEMI; 1000+ long-term follow-up patients). Data from the CRUSADE Registry contributed to three guideline revisions throughout the decade of the 2000s. One of the many important contributions of the CRUSADE Registry was the identification of the relationship between guideline adherence and mortality (Figure 1).

Relationship Between Guideline Adherence (12 Class IA Recommendations) and Mortality.
Reproduced with permission from GR Giugliano, MD.
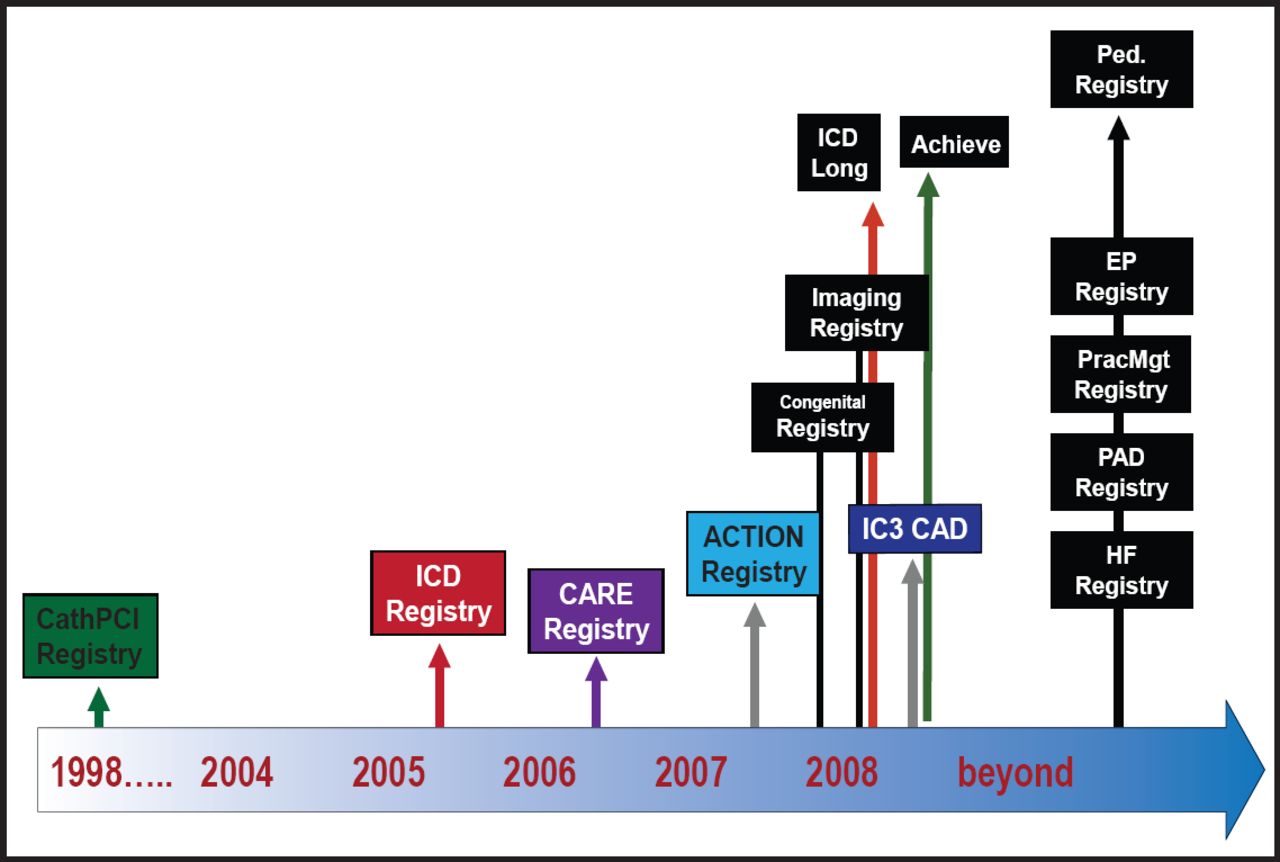
The CRUSADE Registry has been replaced by the ACTION Registry, a component of the National Cardiovascular Data Registry (NCDR™), the most comprehensive, outcomes-based quality improvement program in the US. The NCDR began in 1998 as a single registry but has now grown to comprise five hospital registries (with more planned), representing more than 2200 hospitals nationwide and one clinical practice-based registry (Figure 2). Using the data that were collected, the NCDR has developed clinical modules, programs, and information solutions that support the areas of cardiovascular care in which quality can be measured, benchmarked, and improved.

NCDR.
Reproduced with permission from GR Giugliano, MD.
Registries have been an important source of data, leading to changes in clinical practice. One important contribution has been in the area of bleeding, a critical consideration in the assessment of antithrombotic and interventional therapies. Multivariable analysis of the data that were collected in the CathPCI Registry identified several factors that were related to increased bleeding risk in patients who were undergoing PCI, as shown in Table 1. Several of these risk factors for bleeding, which are now well understood, may not have been identified without the large volume of patients and broad-based data collection that registries make possible (Table 1). Registries also allow for benchmarking between similar institutions using standardized quality-of-care metrics, such as door-to-balloon time. Additionally, real-world data that are related to new devices and drugs can be monitored to identify rare complications or side effects that were not previously documented.
Risk Factors for Bleeding: Adjusted Analysis.
Dr. Giugliano closed with a discussion of the REACH Registry, a global observational study of approximately 68,000 patients in 44 countries who are at high risk of atherothrombosis [Bhatt DL et al. JAMA 2006]. Data from REACH have helped to identify the ethnic and geographical differences in the incidences of cardiovascular risk factors across populations, such as the rates of diabetes and hypertension, differences in age at presentation, and the rates of undertreatment of risk factors in various regions, as well as the overlap among the various forms of vascular disease. In conclusion, Dr. Giugliano encouraged fellow members of the Caribbean Cardiovascular Society to collaborate and support the development of a regional, Caribbean PCI registry with the goal of improving the quality of care that is delivered to CVD patients in the Caribbean through a better understanding of the current risk factors and treatments.
For additional information, please visit: www.ncdr.com.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.