

Summary
This article discusses some of the most recent literature and clinical trials that assessed low-density lipoprotein cholesterol targets and their implications on treatment strategies.
- Lipid Disorders
Cardiovascular disease (CVD) is now the most common cause of death worldwide. While there have been excellent gains in prevention (eg, increased use of aspirin, statins, and other therapies and a reduction in smoking), they have been somewhat tempered by increases in obesity, diabetes, and physical inactivity [Roger VL et al. Circulation 2011]. Robert Giugliano, MD, SM, Harvard Medical School and Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed some of the most recent literature and clinical trials that assessed low-density lipoprotein cholesterol (LDL-C) targets and their implications on treatment strategies.
Although much attention is focused on acute cardiovascular (CV) events, new data show that quiescent, nonobstructive (10% to 30%) but nonetheless “high-risk” nonculprit lesions, in particular those with a thin fibrous cap and significant quantities of underlying cholesterol and lipids, play an important role in future major adverse CV events following percutaneous coronary intervention (PCI) [Stone GW et al. New Engl J Med 2011]. The relationship between lipid levels and coronary artery disease (CAD) is not new. Other mammals and societies that ingest few animal products have very low LDL-C and little CAD [Hochholzer W & Giugliano RP. Ther Adv Cardiovasc Dis 2010].
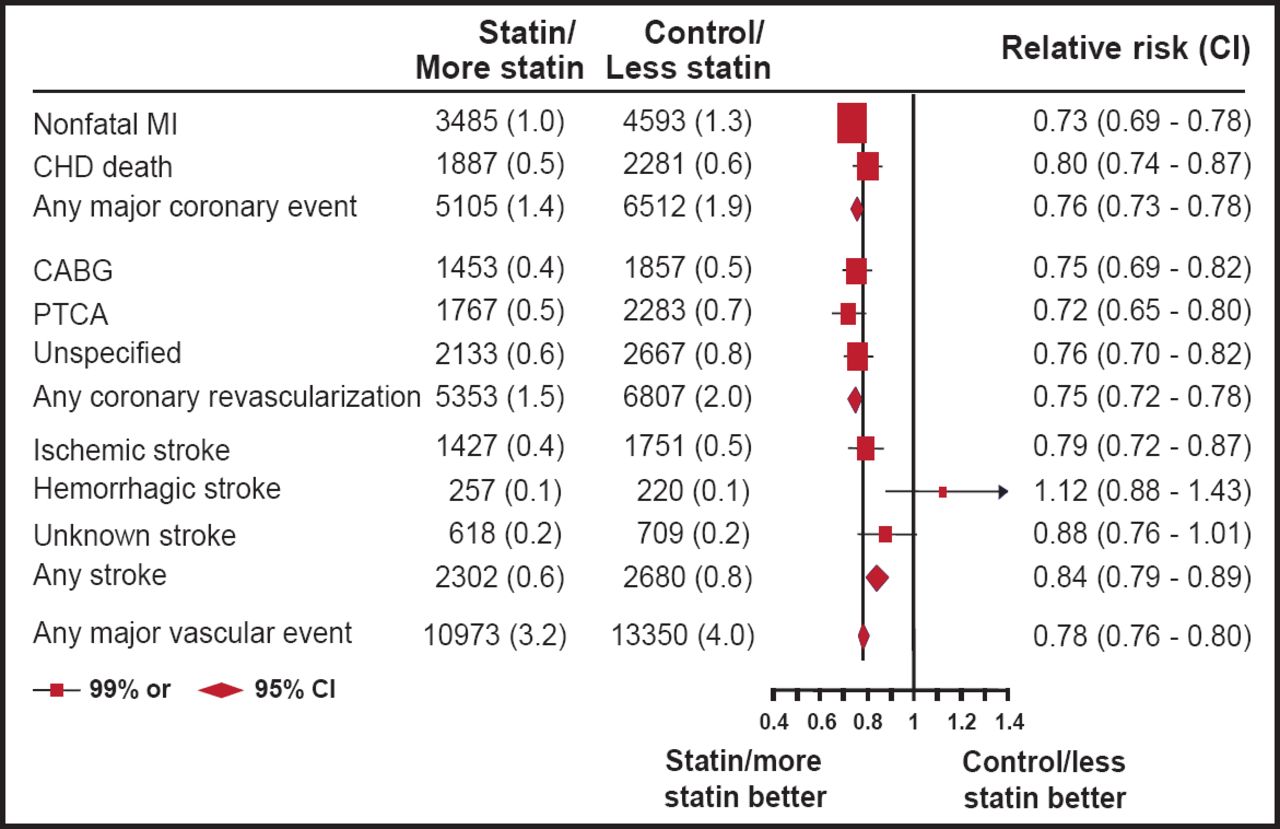
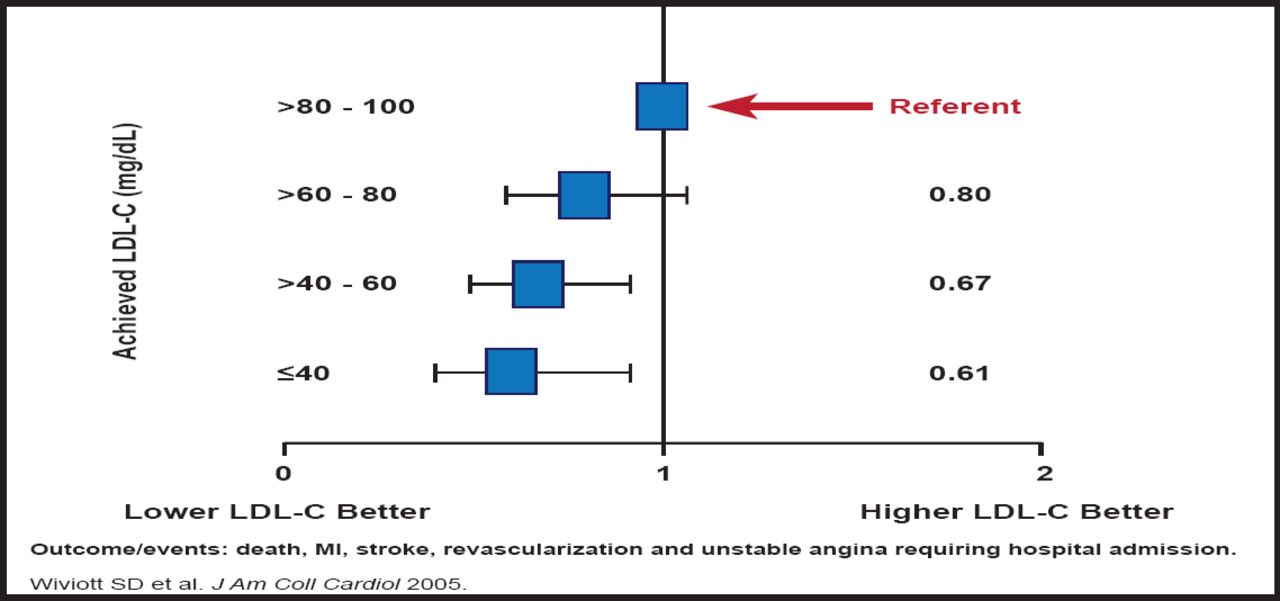
There is also overwhelming evidence from randomized controlled trials that reducing LDL-C reduces CV events. Recent data from Cholesterol Treatment Trialists (CTT) Collaboration [Lancet 2010] indicate that every 1-mM/L (∼40 mg/dL) reduction in LDL-C translates to about a 20% reduction in CV events (Figure 1). The PROVE-IT trial provides support for intensive statin therapy after acute coronary syndrome (ACS). Results from PROVE-IT suggest that achieving LDL-C levels <80 mg/dL (better yet, <40 mg/dL) is associated with improved outcomes, compared with achieving levels of 80 to 100 mg/dL (Figure 2) [Wiviott SD et al. J Am Coll Cardiol 2005]. A recent subanalysis from the JUPITER Trial confirms the benefit of intensive LDL-C lowering, even in patients with already low (≤60 mg/dL) LDL-C at baseline [Hsia J et al. J Am Coll Cardiol 2011]. Both studies also show that intensive therapy is safe. In Dr. Giugliano's opinion, the safety of statin use is related to the dose and choice of drug, not the achieved LDL-C level. Despite lingering fears to the contrary, there is no evidence that statins cause cancer [CTT Collaborators. Lancet 2010].

Key Lessons from Statin Trials.
Reproduced with permission from The Lancet; Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials; Cholesterol Treatment Trialists'; Nov 13, 2010;376(9753):1670–1680.

Better Outcomes with Lower Achieved LDL-C.
Reproduced with permission from the American College of Cardiology; Can Low-Density Lipoprotein Be Too Low? The Safety and Efficacy of Achieving Very Low Low-Density Lipoprotein With Intensive Statin Therapy; Wiviott SD et al. J Am Coll Cardiol 2005;46(8):1411–1416.
Even with all of the data that support positive outcomes with more aggressive cholesterol management, it has been difficult to incorporate these strategies into clinical practice. Approximately 12% of postmyocardial infarction (MI) patients still leave the hospital with without a statin prescription [Kotseva K et al. Lancet 2009], and only 30% of high-risk patients are achieving an LDL-C level <70 mg/dL [Waters D et al. Circulation 2009].
Several promising therapies with different mechanisms and targets are in advanced stages of development: cholesterol absorption inhibitors, cholesteryl ester transfer protein (CETP) inhibitors, and proprotein convertase subtilisin/kexin type 9 (PCSK-9) inhibitors.
Cholesterol Absorption Inhibitors
Dietary cholesterol, absorbed through the intestine and then transported to the liver, is responsible for 25% to 30% of the cholesterol in the body. The remainder is formed by hepatic synthesis. However, as cholesterol is lowered as a result of the effect of statins on hepatic synthesis, the body reacts by increasing cholesterol absorption to maintain its prior ‘balance.’ A new addition to the arsenal of cholesterol-lowering drugs is ezetimibe, a cholesterol absorption inhibitor, which can be used in conjunction with statins to achieve significant LDL-C reductions. Ezetimibe appears to act at the brush border of the small intestine and inhibits the absorption of cholesterol from the intestinal lumen into enterocytes. Use of ezetimibe results in decreased delivery of cholesterol from the intestine to the liver, reduced hepatic cholesterol stores, and increased clearance of cholesterol from the blood. In a 2-week study of 18 hypercholesterolemic patients, ezetimibe inhibited 54% of all intestinal cholesterol absorption compared with placebo (p<0.001) [Sudhop T et al. Circulation 2002]. In patients with chronic kidney disease who did not have an indication for a statin, ezetimibe, in conjunction with simvastatin, reduced the occurrence of major atherosclerotic disease (11.3% for ezetimibe/simvastatin vs 13.4% for placebo; p=0.0022) and vascular events (15.1% vs 17.6%; p=0.0012, ezetimibe/simvastatin and placebo, respectively), beginning in about 1 year. There was no difference in the degree of benefit between nondialysis and dialysis patients, and the combination did not prevent worsening of renal function. There was no increase in the incidence of cancer or the rates of myopathy, liver, or gall bladder events [Baigent C et al. Lancet 2011]. The IMPROVE-IT trial [Cannon CP et al. Am Heart J 2008] is currently studying the effect of simvastatin alone versus ezetimibe/simvastatin in 18,057 ACS patients. The primary study endpoint is CV death, MI, hospital admission for unstable angina, revascularization (>30 days after randomization), or stroke. Patients are being followed every 4 months for a minimum of 4 years. The study is due to report in about 2 years.
CETP Inhibitors
CETP promotes the transfer of cholesteryl esters from high-density lipoprotein cholesterol (HDL-C) to other lipoproteins. Inhibiting this protein raises HDL-C levels and decreases LDL-C levels. The ILLUMINATE trial, which studied torcetrapib, was terminated prematurely due to adverse events in the torcetrapib group [Barter PJ et al. N Engl J Med 2007]. Two other drugs in this class are in late-stage testing: dalcetrapib, currently being evaluated in the Dal-OUTCOMES trial [NCT00658515], which is expected to complete in 2013; and anacetrapib, which is being studied in the REVEAL HPS3-TIMI 55 trial [NCT01252953], which is expected to complete in 2017. While they differ in their effect on LDL-C, both of these drugs, particularly anaceptrapib, have a significant effect on HDL-C (Table 1). In a Phase 2 study in patients with stable coronary heart disease (CHD) or CHD risk equivalent, treatment with anaceptrapib resulted in an almost 40% reduction in LDL-C and a 138% increase in HDL-C [Cannon CP et al. New Engl J Med 2010].
CETP Inhibitors.
PCSK-9 Inhibitors
PCSK-9 inhibitors prevent the destruction of LDL receptors by PCSK-9, allowing more LDL to be removed from the blood. They have been shown to achieve LDL-C reductions of more that 60% [Swergold G et al. AHA 2010] with injections that can last up to 4 weeks. These are extremely potent drugs that can achieve LDL-C levels in the teens and are most effective when given in combination with a statin.
In concluding, Dr. Giugliano said that there is now overwhelming data from randomized controlled trials that reducing LDL-C with statins reduces CV events and new data that support that LDL-C targets as low as <70 mg/dL are safe and even more effective in reducing CV events. Several promising therapies with different mechanisms and targets are in advanced stages of development.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.