

Summary
Although the ability to measure cardiac troponin quickly and accurately has improved the cardiologist's ability to detect myocardial injury in the setting of acute coronary syndrome, there are a variety of noncoronary cardiac conditions that also lead to elevated troponin concentrations.
- Myocardial Infarction
The Joint European Society of Cardiology/American College of Cardiology (ESC/ACC) Committee's 2007 consensus document for the redefinition of myocardial infarction (MI) places significant emphasis on the detection of troponin T and troponin I [Thygessen. Eur Heart J 2007]. Although the ability to measure cardiac troponin quickly and accurately has improved the cardiologist's ability to detect myocardial injury in the setting of acute coronary syndrome (ACS), there are a variety of noncoronary cardiac conditions that also lead to elevated troponin concentrations. Christian W. Hamm, MD, Kerckhoff Klinik, Bad Nauheim, Germany, discussed the implications of elevated troponin concentration in patients with noncoronary cardiopulmonary conditions, such as myocarditis, congestive heart failure, pulmonary embolism, and septic shock and in critically ill patients in whom there is myocardial necrosis but not necessarily ST or non-ST elevation myocardial infarction.
An elevated troponin concentration is relatively common in critically ill patients and is strongly predictive of adverse outcomes. Compared with patients who have ACS, critically ill patients without ACS but with an elevated troponin concentration have poorer outcomes [Alcalai R et al. Arch Intern Med 2007]. In patients with congestive heart failure, an elevated troponin concentration is correlated with the severity of symptoms and is more frequently detected in patients with NYHA class III or IV compared with class II symptoms (p=0.02). Patients with severe heart failure and elevated troponin have significantly worse outcomes than similar patients with no troponin elevation [Setsuta K et al. Am J Med 2002]. Similar findings have been reported for patients with myocarditis [Smith SC et al. Circulation 1997]. Troponin may also improve risk stratification in pulmonary embolism, as in-hospital death, prolonged hypotension, cardiogenic shock, and the need for resuscitation have been associated with elevated troponin concentration [Giannitsis E et al. Circulation 2000].
Low-level troponin elevations have been observed in patients with chronic renal failure. However, in this setting, the elevation is generally characterized not by a rise and fall (which is typical with ACS) but a constant elevation. Outcomes have been associated with the degree of elevation in this population, with a greater-than-7-fold increase in mortality risk when concentrations of cardiac troponin T reach levels >0.10 ng/mL [Dierkes J et al. Circulation 2000]. This prognostic ability of troponin T is retained, regardless of the creatinine clearance level, an indicator of kidney function [Aviles RJ et al. N Engl J Med 2002].
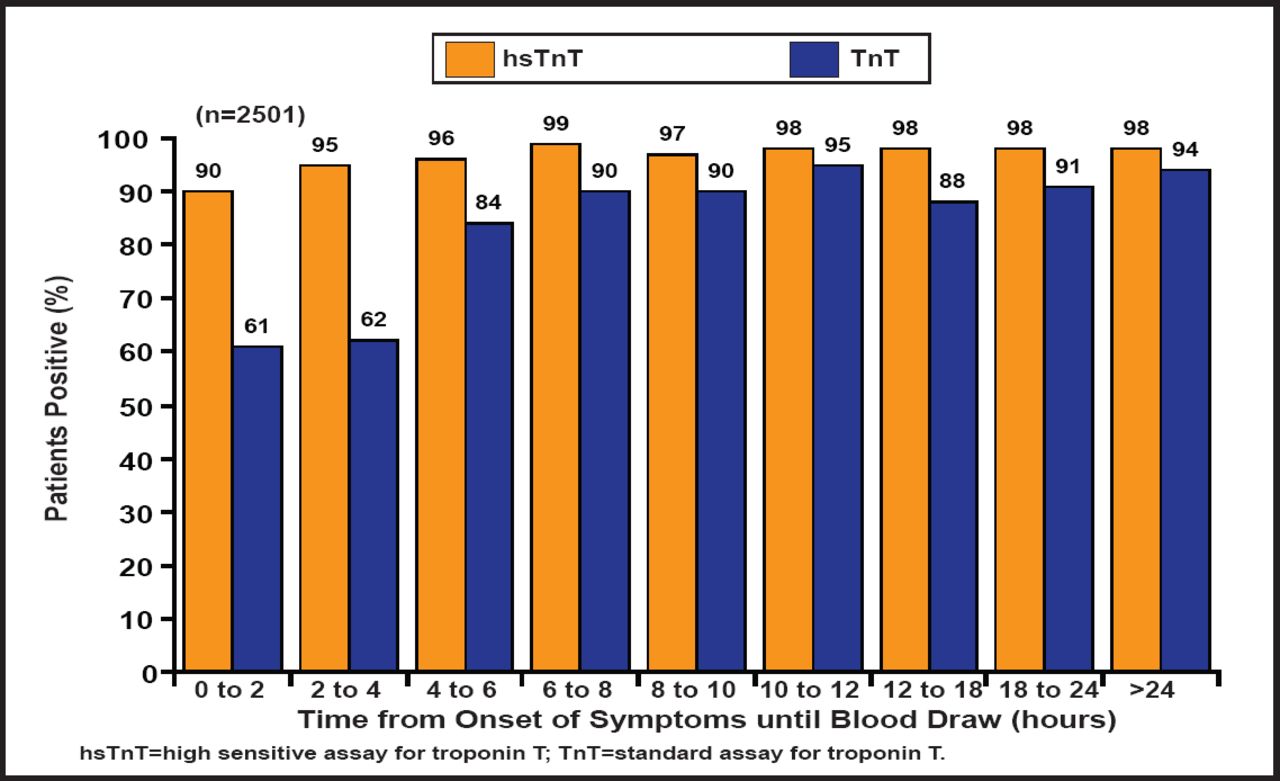
Improvements in the analytical performance of current-generation troponin assays have led to better prognostic assessment. The fourth- and fifth-generation assays are now 10 to 15 times more sensitive and are capable of detecting troponin within the first 2 hours of symptom onset in 90% of patients with MI compared with 61% of patients, using the older standard assays (Figure 1) [Weber M et al. Am Heart J 2011]. The ESC/ACC Consensus Document states the troponin assay performance must be in the 99th percentile of the reference control group and have a coefficient of variation ≤10% [Alpert JS. Eur Heart J 2000]. There are four assays, two each for troponin T and I, that satisfy this requirement.

High-Sensitivity Assay Troponin T in AMI.
hsTnT = high-sensitivity assay for troponin T; TnT = standard assay for troponin T; “Reprinted from the American Heart Journal, Weber M et al, Improved diagnostic and prognostic performance of a new high-sensitive troponin T assay in patients with acute coronary syndrome. July 2011;162(1):81–88, with permission from Elsevier.
Cardiac troponin remains the preferred biomarker of myocardial injury and a central component in the diagnosis of myocardial infarction. Troponin, even at low-level elevations, remains one of the most powerful prognostic biomarkers across a variety of clinical settings. Analytical improvements in assay performance, however, have enabled the detection of myocardial injury at very low levels and in an increasing number of patients with diagnoses other than ACS. The increased frequency of detection and the decreased specificity for ACS have presented a challenge for clinicians. Consideration of the specific clinical context is critical in interpreting the significance of an elevated troponin concentration and understanding the therapeutic implications.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.