

Summary
The benefits of calcium intake for bone health are very clear, but the risks—cardiovascular (CV), in particular—have become controversial. This article discusses calcium metabolism and the results of recent studies on calcium supplementation and CV health.
- metabolic bone disease
The benefits of calcium intake for bone health are very clear, but the risks—cardiovascular (CV), in particular—have become controversial. Richard Bockman, MD, PhD, Weill Cornell Medical College and Hospital for Special Surgery, New York, New York, USA, discussed calcium metabolism and the results of recent studies on calcium supplementation and CV health.
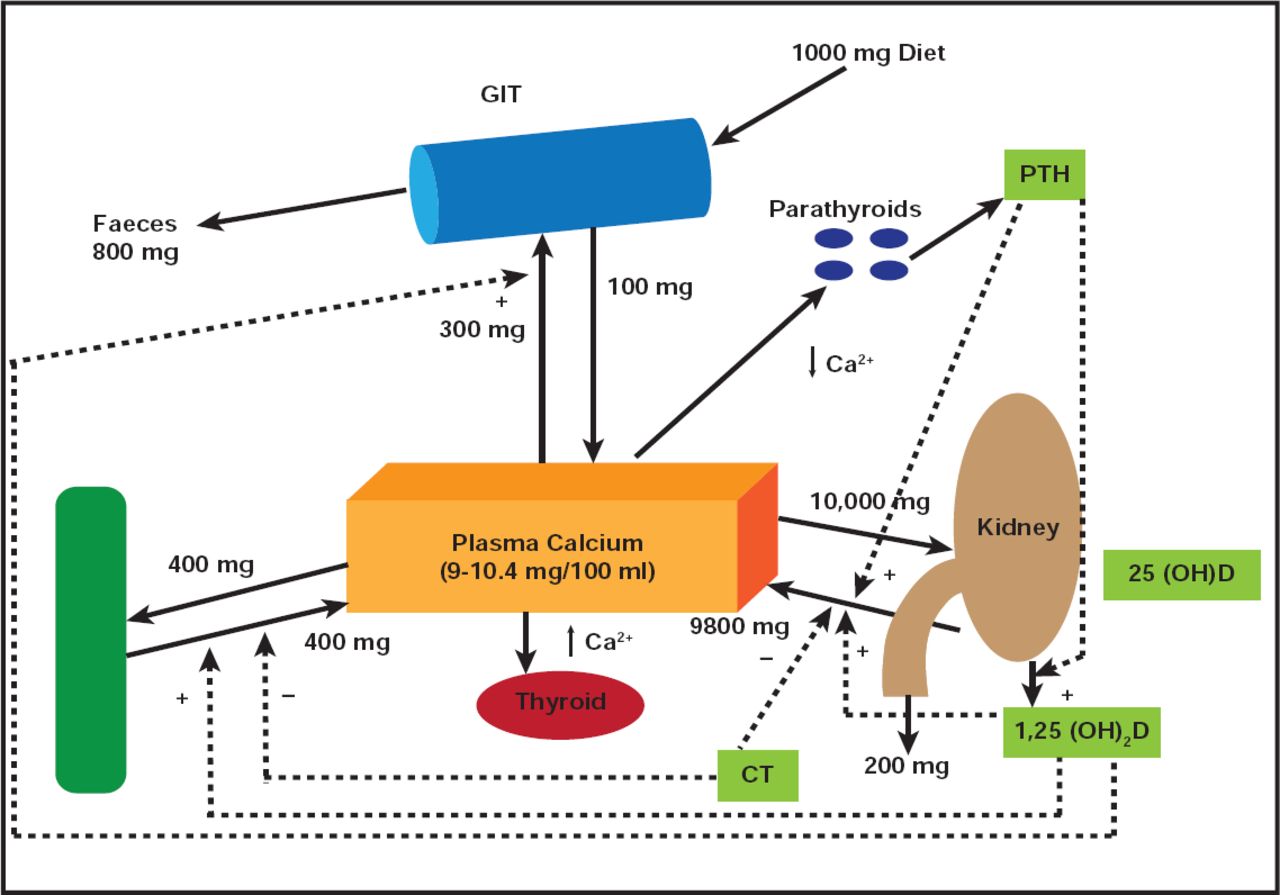
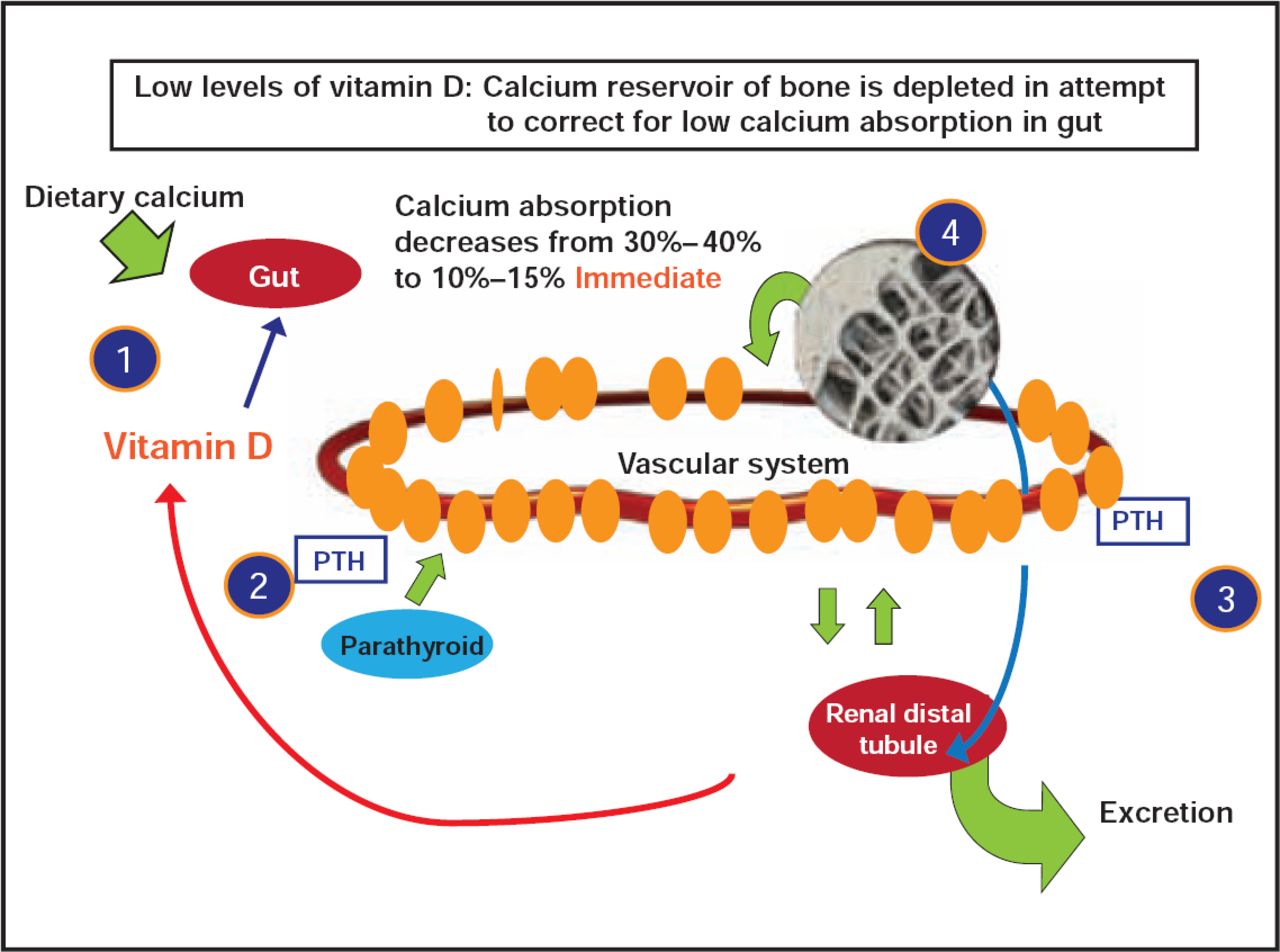
According to Dr. Bockman, calcium is anything but a solitary player in nutrient metabolism. “It isn't about Ca, D, P, PTH (parathyroid hormone), or FGF 23 (fibroblast growth factor 23),” he said. “It's about all of them interacting” (Figure 1). Dr. Bockman reports that when vitamin D status is sufficient, absorption of dietary calcium is approximately 30% to 40%. As vitamin D status declines, absorption of dietary calcium drops to approximately 10% to 15% (Figure 2). Low levels of calcium and vitamin D lead to increased release of PTH. This raises bone resorption and decreases bone mass.

Calcium Metabolism.
Reproduced with permission from R. Bochman, MD, PhD.

Interaction of Calcium, Vitamin D, and PTH with Bone and Kidney.
Reproduced with permission from R. Bochman, MD, PhD.
Given its effect on calcium absorption, vitamin D and calcium insufficiency are associated with bone loss and increased fracture risk. Excessive P alters D, FGF, and intact PTH and increases bone loss.
Recently, the safety of calcium intake has become controversial, based on reports of increased risk of CV events that are associated with calcium supplementation (143 vs 111; HR, 1.31; 95% CI, 1.02 to 1.67; p=0.035) [Bolland MJ et al. BMJ 2010; Bolland MJ et al. BMJ 2011]. Bolland's meta-analysis from 2010 included novel datasets that were obtained from the principal investigators after the published reports, with CV outcomes obtained from self-reports, hospital admissions, and death certificates. Fifteen randomized controlled trials were eligible for inclusion—five with patient-level data and six with partially complete trial-level data.
The opposing view that calcium supplementation does not increase CV risk has also been published recently [Lewis et al. JBMR 2010]. A systematic review and meta-analysis by Wang et al. [Ann Intern Med 2010] found no increased CV risk that was associated with calcium supplementation. The authors excluded ecological, cross-sectional, and retrospective case control studies, as well as studies that did not ascertain cardiovascular disease (CVD) events (including CVD death, nonfatal coronary heart disease, myocardial infarction, and nonfatal stroke). The meta-analysis included only original study data, in which compliance was >80% and outcomes were formally collected.
According to the Institute of Medicine's review of calcium supplementation and CV risk, most studies in the meta-analyses were small and did not report dietary calcium. Vascular events were not studied as a primary outcome and were not always adjudicated. In many cases of CV events, the confidence intervals included the null association value of one. In addition, renal function was not considered a covariate in the studies, which is a well-known risk factor for CVD [Institute of Medicine: Dietary reference intakes for calcium and vitamin D. In: Washington, DC. The National Academies Press 2011].
A true placebo-controlled, randomized trial of a single, readily available nutrient, such as calcium, is often difficult to achieve. Compliance with study parameters must be maintained at levels well above 80% to provide confidence in a verifiable outcome. Clear, definable endpoints that can be validated must be used, and the most stringent methods of statistical analysis must be applied in order to provide a final answer to this complex question. Until then, the preponderance of evidence does not point to a definite conclusion regarding calcium supplementation as a cause of CV events.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.