

Summary
Researchers recommended widespread adoption of a program that eliminates copayments for preventive medications after the Post-Myocardial Infarction Free Rx Event and Economic Evaluation trial [MI FREEE; NCT00566774] showed that the policy improved treatment adherence without increasing overall health costs.
- Myocardial Infarction Clinical Trials
Researchers recommended widespread adoption of a program that eliminates copayments for preventive medications after the Post-Myocardial Infarction Free Rx Event and Economic Evaluation trial [MI FREEE; NCT00566774] showed that the policy improved treatment adherence without increasing overall health costs. The outcomes from the trial were presented by Niteesh K. Choudhry, MD, PhD, Harvard Medical School, Boston, Massachusetts, USA.
The investigator-initiated, cluster-randomized, controlled policy study enrolled patients who were discharged after myocardial infarction (MI) and randomly assigned by their insurance plan sponsors to full or usual prescription coverage for all statins, β-blockers, angiotensin-converting enzyme inhibitors, or angiotensin-receptor blockers. Antiplatelet therapy was not included. The randomization was by plan sponsor (ie, employer, union, government, association) and not by patient. The primary outcome was the first major vascular event or revascularization. Secondary outcomes were rates of medication adherence, total major vascular events or revascularization, the first major vascular event, and pharmacy and medical spending.
Patients were eligible for inclusion if they received both medical and prescription drug benefits through Aetna, a large commercial insurer in the United States, and if they had been discharged from the hospital with a diagnosis of MI and had a length of stay of between 3 and 180 days. They were excluded if they were enrolled in a health savings account or if they were aged ≥65 years at the time of discharge [Choudhry NK et al. Am Heart J 2008].
A total of total 2845 patients (1494 plan sponsors) were randomized to full prescription coverage, and 3010 patients (1486 plan sponsors) were given usual coverage. The mean time between the index event and randomization was 49 days. The majority of patients (94%) underwent angiography for their index event, with 67% receiving PCI.
Adherence for all three types of medications combined was higher in the full coverage group compared with the usual coverage group (43.9% vs 38.9%; p<0.001). When looked at individually, there were higher rates of compliance with each medication with full coverage compared with usual coverage, with rates of adherence ranging from 35.9% to 49% in the usual coverage group and 4 to 6 percentage points higher in the full coverage group (p<0.001 for all comparisons).
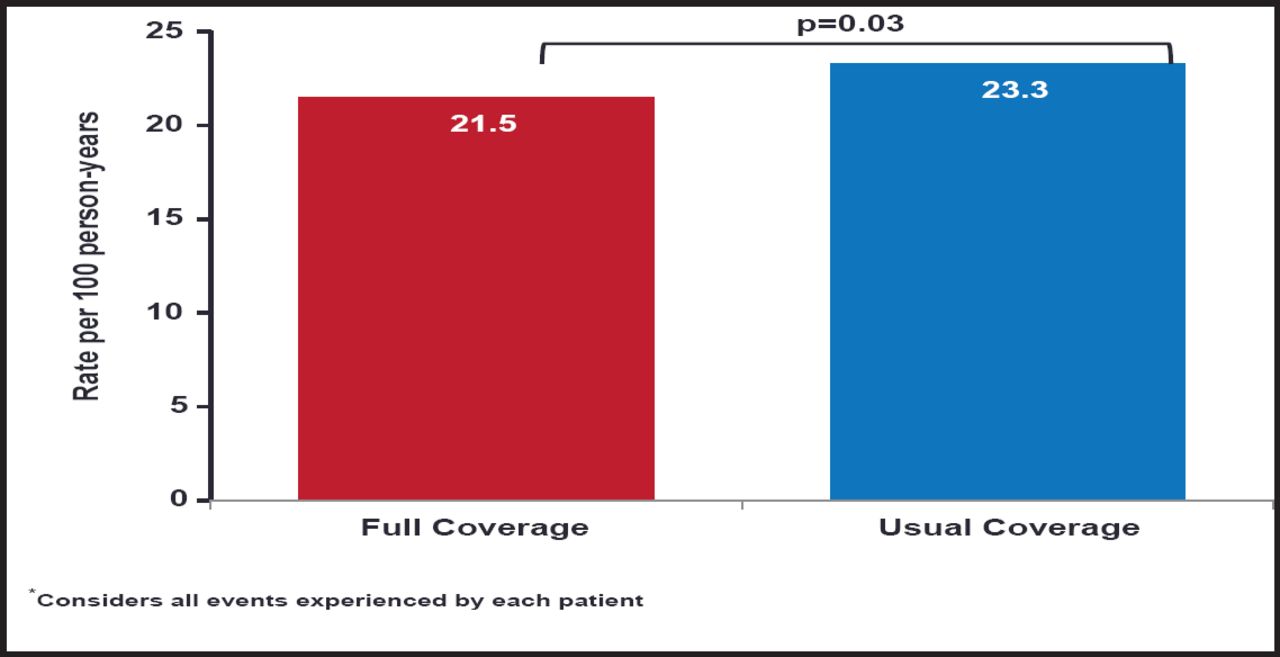
There was no significant between-group difference in the primary outcome (17.6 per 100 person-years in the full coverage group vs 18.8 in the usual coverage group; HR, 0.93; 95% CI, 0.82 to 1.04; p=0.21). However, rates of secondary endpoints, including total major vascular events and revascularization (includes recurrent events), were significantly reduced in the full coverage group (21.5 vs 23.3; HR, 0.89; 95% CI, 0.90 to 0.99; p=0.03; Figure 1), as was the rate of first major vascular event (11.0 vs 12.8; HR, 0.86; 95% CI, 0.74 to 0.99; p=0.03).

Total Major Vascular Events or Revascularization.
Reproduced with permission from N. Choudhry, MD, PhD.
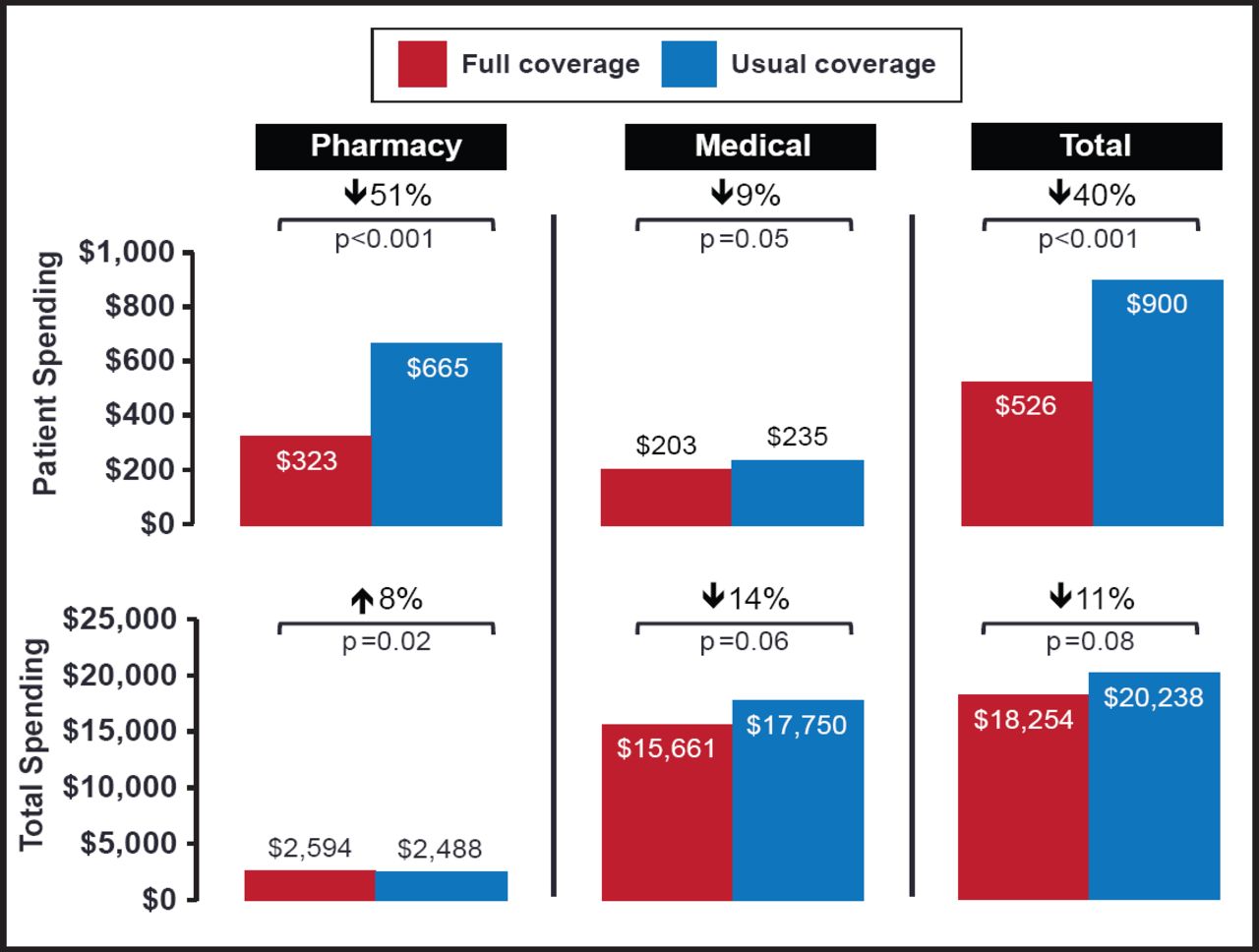
Elimination of copayments did not increase total spending ($66,008 for the full coverage group vs $71,778 for the usual coverage group; relative spending, 0.89; 95% CI, 0.50 to 1.56; p=0.68), but patient costs were significantly reduced for drugs and other services (relative spending, 0.74; 95% CI, 0.68 to 0.80; p<0.001; Figure 2).

Cardiovascular Spending.
Reproduced with permission from N. Choudhry, MD, PhD.
Adherence to medications that were prescribed post-MI was poor. Although it was significantly greater for all categories of medication among patients with no out-of-pocket costs (p<0.001 for all comparisons), that absolute increase was modest (only 4% absolute increase), and rates still remained low, reaching a mean adherence of <50% in all medication classes. Dr. Choudhry noted that the results highlight the need for other interventions to promote adherence—eg, ones that target such causes as complex treatment regimens, difficulties in accessing medications, knowledge gaps, adverse effects, and forgetfulness.
Results of MI-FREE demonstrate that adherence can be modestly improved by eliminating copays. Possible explanations for the lack of associated clinical benefit include that only a subset of medications were covered (eg, no antiplatelet therapy) and that patients were distant from their index event before randomization (mean 49 days). Overall, these results are important and promising, as patient adherence is recognized as an important and complex component of improving outcomes. Further investigation will be important in understanding the optimal payment strategy to maximize patient adherence.
- © 2011 MD Conference Express®
Further Reading
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.