

Summary
Guidelines and scientific statements inform practitioners and patients about appropriate health care for specific clinical circumstances. This article reviews the process for the development of Stroke Council guidelines and highlighted recent updates.
- Nursing
- Cerebrovascular DiseaseThrombotic Disorders Guidelines
- Ischemia
- Prevention & Screening
Guideline and Scientific Statement Development
Guidelines and scientific statements inform practitioners and patients about appropriate health care for specific clinical circumstances. Colin P. Derdeyn, MD, Washington University School of Medicine, St. Louis, Missouri, reviewed the process for the development of Stroke Council guidelines and highlighted recent updates. Dr. Derdeyn currently chairs the Stroke Council's Scientific Statements Oversight Committee (SOC).
Six core guidelines, based on expert review of current scientific evidence, are updated every 3 years and are intended to assist health care providers in clinical decision-making by describing a range of generally acceptable approaches for the diagnosis, management, or prevention of specific conditions related to stroke. Specific objectives are to improve patient outcomes, reduce practice variation, influence policy, and promote efficient resource utilization. Scientific statements are focused on a particular practice- or research-oriented issue and are updated as needed. Advisories are updates, based on recent trials that change a practice guideline recommendation and need to be disseminated before a scheduled full guideline update.
Three of the six core stroke guidelines were published in 2010–2011 and include those concerning the primary prevention of stroke, the prevention of stroke in patients with stroke or transient ischemic attack (TIA), and the management of spontaneous intracerebral hemorrhage (ICH). Updated versions for the remaining three guidelines—early management of acute ischemic stroke, management of subarachnoid hemorrhage, and stroke rehabilitation—are in development.
Any physician can propose an idea for scientific statement development. Once the SOC agrees to the concept, the scope, the objectives, and the writing group are developed with the American Heart Association (AHA) Manuscript Oversight Committee. All guidelines undergo internal peer-review. After the AHA Scientific Advisory Coordinating Committee approves the final version of a stroke-related guideline, it is published online and in Stroke. Full disclosure is required from all authors, reviewers, and chairs.
Dr. Derdeyn noted that that guidelines are not commandments, and the final judgment regarding the care of a specific patient must be made in light of circumstances that are unique to that patient and clinical expertise.
Diagnosis and Management of Cerebral Venous Thrombosis
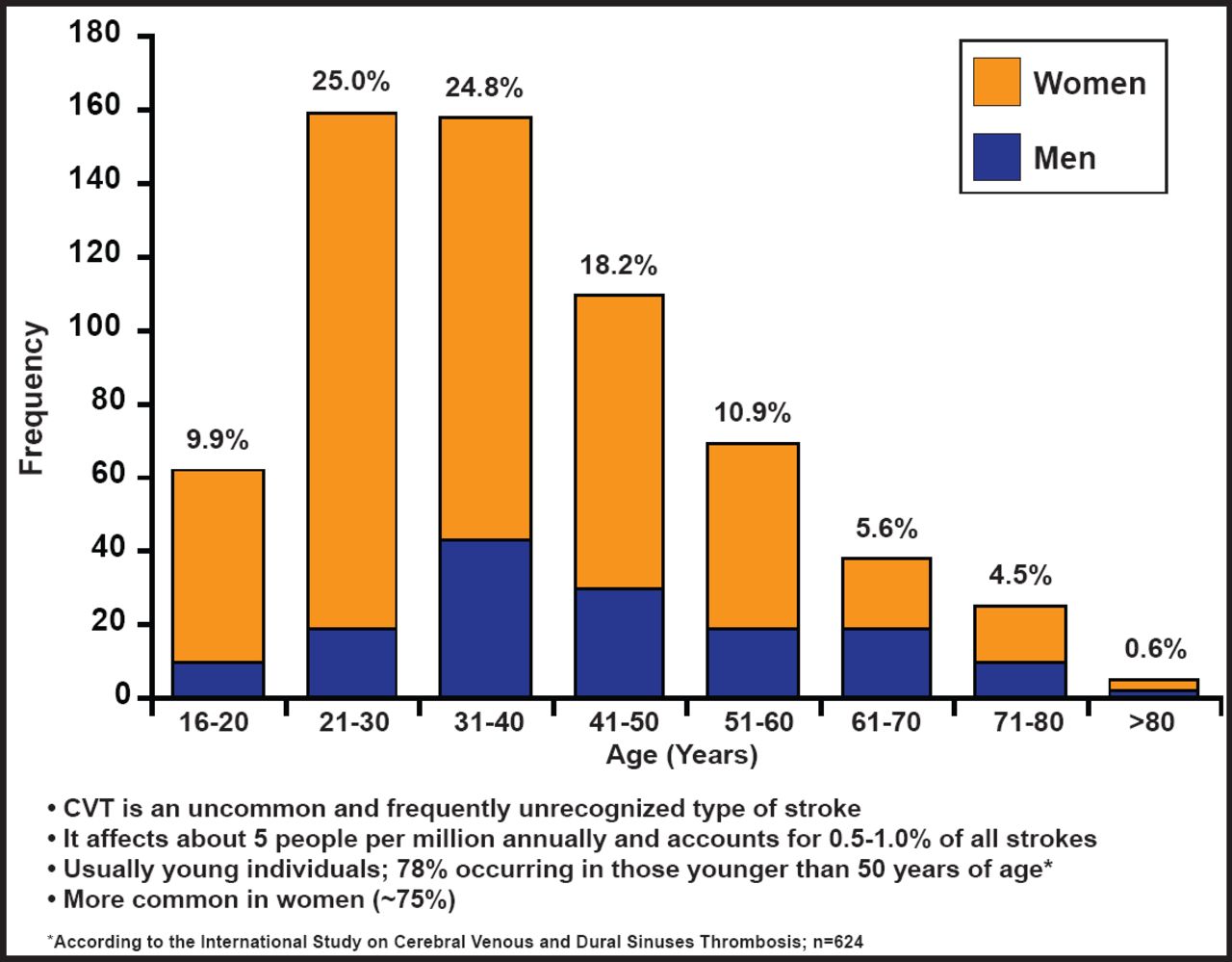
Cerebral venous thrombosis (CVT) is an uncommon and frequently unrecognized type of stroke that accounts for 0.5% to 1% of all strokes, 5% of all cases of ICH, and is more frequent in women aged <50 years. Gustavo Saposnik, MD, St. Michael's Hospital, Toronto, Canada, presented evidence-based AHA Stroke Council recommendations for the diagnosis, management, and treatment of CVT (Figure 1).

Epidemiology and Risk Factors.
Reproduced with permission from C. Derdeyn, MD.
The diagnosis of CVT is typically based on clinical suspicion and imaging. Diffused and often progressive headaches are present in nearly 90% of patients. Focal or generalized seizures may occur in about 40% of patients. The most common area that is affected is the superior sagittal sinus.
Diagnostic imaging of CVT with CT or MRI can be used to identify a filling defect within the vein or sinus and to determine vascular and parenchymal changes. CT is widely used as the initial imaging test in patients who present with new-onset neurological symptoms. The primary sign of acute CVT in one-third of patients who are imaged with CT is hyperdensity of a cortical vein and/or dural sinus, while the absence of a flow void and signal intensity of the sinus are signs that are used to detect CVT with noncontrast enhanced MRI. Class I/II evidence suggests the use of imaging of the central venous system to exclude CVT in patients with the clinical features of idiopathic intracranial hypertension or those with headache that is associated with atypical features.
Treatment guidelines recommend initial anticoagulation therapy with adjusted-dose unfractionated heparin or weight-based low-molecular-weight heparin, early initiation of antiepileptic drugs in patients with seizures and parenchymal abnormalities (eg, hemorrhage, venous infarction), and monitoring for progressive visual loss; steroid medications are not recommended. In the absence of seizures, routine use of antiepileptic drugs is not recommended.
In addition to the above, the guidelines provide recommendations for the evaluation and management of CVT during pregnancy and in pediatric populations. Considerations for the management of clinical complications (seizures, hydrocephalus, intracranial hypertension, and neurological deterioration) are also summarized.
Intracerebral Hemorrhage Guidelines
J. Claude Hemphill, III, MD, San Francisco General Hospital, San Francisco, California, noted there are no approved treatments for ICH for which a proven benefit in decreasing morbidity or mortality has been shown in a Phase III trial. Despite this, it is known that aggressive care of ICH is associated with better outcomes; therefore, guidelines are valuable as assessments of current treatments, educational tools, and a framework for future directions.
Regarding coagulopathy related to warfarin use, the guidelines recommend using a standardized protocol: using prothrombin complex concentrates or fresh frozen plasma in addition to vitamin K, focusing on ultra-early treatment, and tracking usage related to outcome and cost. The usefulness of platelet transfusions in ICH patients with a history of antiplatelet use is unclear and is considered investigational. Because of conflicting evidence concerning poor outcomes and the lack of information on the utility of reversal strategies, Dr. Hemphill recommends using best judgment and staying current with emerging data. Because the FAST trial [Mayer SA et al. New Engl J Med 2008] did not show an outcome benefit for rFVIIa and in light of its association with an increased thromboembolic risk, rFVIIa is not recommended in unselected patients without coagulopathy. There have been no changes in the blood pressure guidelines since 2007; thus, following the current guidelines is recommended.
Although current guidelines recommend treating convulsive and nonconvulsive seizures with antiepileptic drugs, new recommendations suggest using EEG for patients with decreased levels of consciousness of unclear etiology and not using prophylactic anticonvulsants, particularly phenytoin. The guidelines for surgical hematoma evacuation have changed somewhat from the 2007 guidelines because of ongoing consideration of the impact of the Surgical Trial in Intracerebral Hemorrhage (STICH) Study, [Jones RH et al. New Engl J Med 2009] which suggested no difference in outcome between early surgery (∼30 hours after onset) and conservative medical treatment. The guidelines regarding the withdrawal of support have been revised and now suggest aggressive full care early after ICH onset and postponement of new DNR orders until at least the second full day of hospitalization.
Dr. Hemphill concluded that “guidelines are not a cookbook, nor a substitute for clinical expertise” and clinicians “don't have to follow the 2010 AHA/ASA ICH guidelines, but if you don't, you need to defend why you aren't.”
Primary Prevention of Stroke: What's New?
Larry B. Goldstein, MD, Duke University Medical Center, Durham, North Carolina, discussed highlights of the new primary stroke prevention guidelines concerning lifestyle, carotid revascularization, atrial fibrillation (AF), and primary prevention in the emergency department.
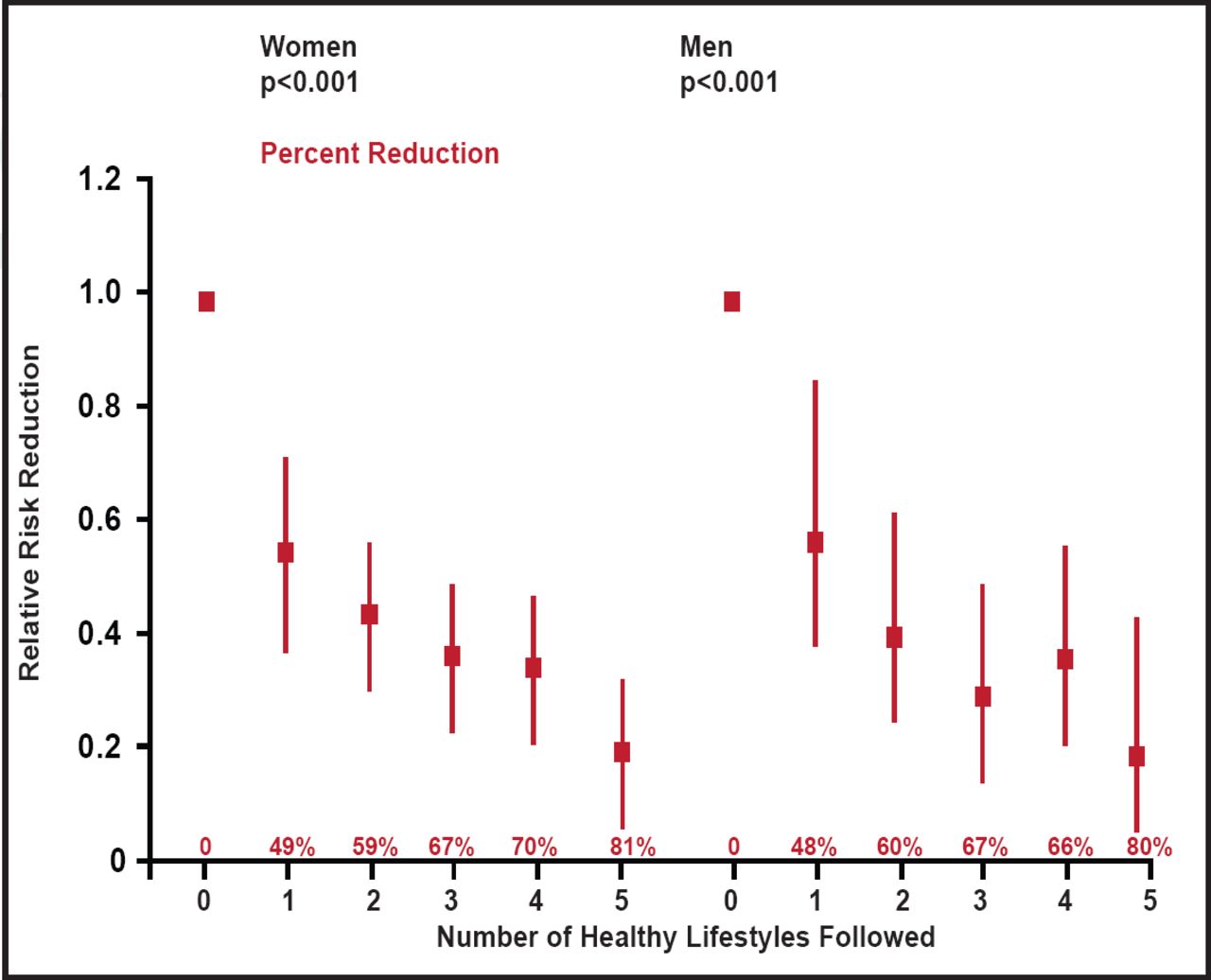
Based on a recent study [Chiuve SE et al. Circulation 2008], the following lifestyle choices were identified as important factors for reducing the risk of a first stroke: not smoking, healthy diet, ≥30 min per day of moderate or vigorous physical activity, maintaining BMI <25 kg/m2, and having no more than 1 (nonpregnant women) or 1 to 2 (men) alcoholic drinks per day. Women and men who adhere to these “healthy” lifestyles have an approximately 8% lower risk of stroke as compared to those who do not (Figure 2).

Impact of Healthy Lifestyle and Risk of First Stroke.
Chiuve SE et al. Primary Prevention of Stroke by Healthy Lifestyle. Circulation. 28 August 2008; 118:904–906.
Previous clinical trials show the benefits of carotid endarterectomy in reducing the incidence of a first ischemic stroke in patients with substantial carotid artery narrowing [ACAS Executive Committee. JAMA 1995; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Lancet 2004]. The current guidelines downgrade the strength of the recommendation for endarterectomy, based on apparent reductions in the rate of stroke with medical therapy alone [Abbott AL. Stroke 2009]. Based on this, it was also noted that the 3% complication rate threshold is likely too high, although the operation might still be beneficial for carefully selected patients with significant carotid stenosis (minimum 60% by angiography, 70% by validated Doppler ultrasonography). In the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), the risk of the composite primary outcome of stroke, myocardial infarction, or death did not differ significantly between groups that underwent carotid artery stenting and those who underwent carotid endarterectomy [Brott TG et al. N Engl J Med 2010]. It was noted, however, that the overall rate of stroke was approximately twice that of endarterectomy. The Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy Trial (SAPPHIRE) showed that among patients with severe carotid artery stenosis and coexisting conditions, carotid stenting with the use of an embolic protection device was not inferior to carotid endarterectomy [Yadav JS et al. N Engl J Med 2004]. The event rates in both groups were considerably higher than what would be expected with medical therapy alone. The new guidelines note that the value of carotid revascularization for patients with asymptomatic carotid stenosis as compared with medical therapy is not well established.
Oral anticoagulation therapy reduces the risk of vascular events in patients with AF. The Atrial Fibrillation Clopidogrel Trial With Irbesartan for Prevention of Vascular Events (ACTIVE W; NCT00243178) established that oral anticoagulation therapy was superior to clopidogrel plus aspirin for the prevention of vascular events in patients with AF who are at high risk of stroke [ACTIVE Investigators. Lancet 2006]. In patients with AF for whom vitamin K antagonist therapy was unsuitable, the addition of clopidogrel to aspirin reduced the risk of stroke, but this was balanced by an increase in the risk of major hemorrhage [ACTIVE A Trial; NCT00249873; ACTIVE Investigators. N Engl J Med 2009]. Thus, the guidelines indicate that for high-risk patients with AF who are deemed unsuitable for anticoagulation, dual antiplatelet therapy with clopidogrel and aspirin offers more protection against stroke than aspirin alone but with an increased risk of major bleeding.
Opportunities for primary prevention of stroke in the emergency department include educating patients about smoking cessation programs and interventions, identification of AF and initial evaluation for anticoagulation, screening for hypertension, and referral to an appropriate therapeutic program in the case of drug or alcohol abuse. The effectiveness of screening, brief intervention, and referral for treatment of diabetes and lifestyle stroke risk factors in the emergency department setting has not yet been established.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.