

Summary
In the late 1990s, the American Heart Association set a goal to reduce the rates of individual cardiovascular risk factors as well as death from CV causes by 25% by 2010. This article discusses the latest results on progress toward reaching those goals.
- Prevention & Screening
In the late 1990s, the American Heart Association (AHA) set a goal to reduce the rates of individual cardiovascular (CV) risk factors as well as death from CV causes by 25% by 2010. Daniel W. Jones, MD, University of Mississippi, Jackson, MS, reported the latest results on progress toward reaching those goals.
By 2007, this goal had been achieved in three areas: the death rate from coronary heart disease had been reduced by 38%, the rate of strokes was down by 33%, and the percentage of individuals with uncontrolled high blood pressure was 28% lower. Progress was also being made toward meeting this goal for three additional risk factors; high cholesterol, smoking prevalence, and the number of individuals who were not engaged in moderate or vigorous physical activity were down 22%, 20%, and 9%, respectively.
The committee decided that the goal of a 25% reduction in diabetes and obesity was unattainable. Just stopping the growth of these two diseases would be significant progress, so they reset the target to 0% growth by 2010. The most recent data indicate a 1.9% annual growth rate for obesity and 1.8% for new diabetes. Good progress has been made toward the 2010 goal of reducing mortality and high blood pressure, fair progress has been made toward achieving the cholesterol goal, while poor progress has been made with changing the lifestyle issues, concluded Dr. Jones.
As reported by Donald M. Lloyd-Jones, MD, Northwestern University, Chicago, IL, the new goal commits AHA to the following: “By 2020, to improve the cardiovascular health of all Americans by 20% while reducing death from cardiovascular disease and stroke by 20%.”
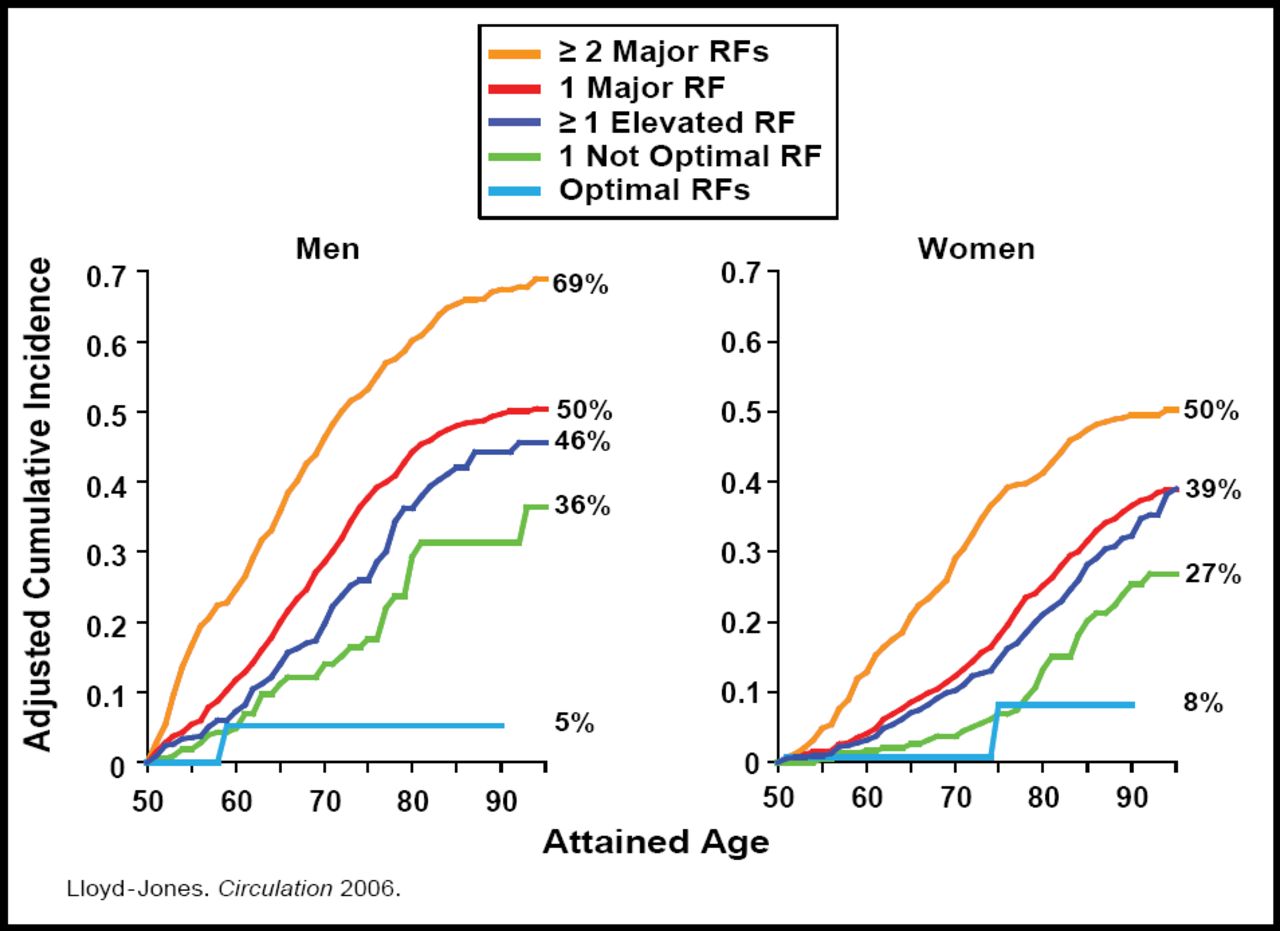
Dr. Lloyd-Jones noted that studies indicate that a lower risk factor burden in middle age is associated with very low remaining lifetime risk for CV and other diseases (Figure 1) [Lolyd-Jones D. Circulation 2006], markedly longer survival, greater health-related quality of life, and substantially decreased Medicare expenditures in older ages. The fewer the lifestyle or other risk factors someone has, the greater their reduction in CVD risk. Thus, the focus for the CV health metric has shifted toward synthesizing and incorporating the entire spectrum of CV health, with ideal CV health as the ultimate goal. The new mission offers opportunities for preventing risk factor development in the first place, while also controlling risk once it exists, treating disease, and improving quality of life in those with chronic illness. By providing opportunities for greater clinical prevention and public health approaches, new challenges and prospects will be made available for expansion in the area of primordial prevention (in particular, the prevention of risk factors in children and younger adults).

Lifetime Risk: Age 50.
An improved diet is a critical component of the AHA's strategy for CVD risk reduction in the AHA Impact 2020 project. Lawrence Appel, MD, Johns Hopkins University, Baltimore, MD, reviewed the dietary components that have a potential to prevent disease and improve CV health. The AHA dietary guidelines and recommendations are consistent with the Dietary Approaches to Stop Hypertension (DASH), Okinawa, and Mediterranean diets. The five key components of the diet involve the consumption of more fruits, vegetables, oily fish, and fiber and less sodium and sugar. Data for US residents indicate that very few adults or children achieve optimal levels for at least 4 of these foods and nutrients—just 0.6% for adults and 0.1% for children (Table 1).
Prevalence of Adherence to Healthy Diet Score (NHANES 2005–6).
The AHA 2006 Diet Guidelines recommend the consumption of a variety of foods within and among the basic food groups while staying within energy needs; the control of caloric intake to manage body weight; physical activity every day; increased daily intake of fruits and vegetables, whole grains, and fibrous foods; reduced-fat milk and milk products; limited intake of saturated and trans fats; the use of small amounts of salt and sugar; and reduced alcohol intake. Greater adherence to these and similar diet guidelines is associated with a significant reduction in mortality from all causes [Trichopoulou A et al. N Engl J Med 2003; Fung TT et al. Arch Intern Med 2008].
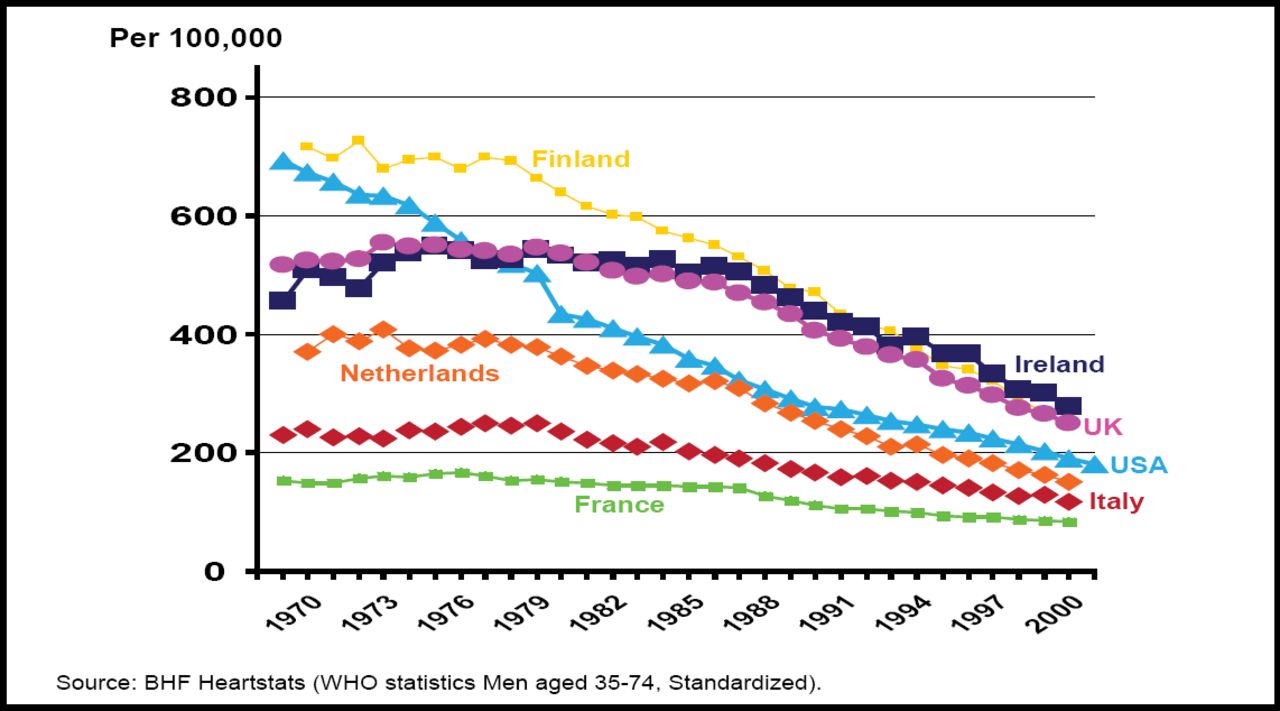
Between 1968 and 2003, mortality rates from coronary heart disease (CHD) declined by approximately 50% in many countries. Darwin R. Labarthe, MD, PhD, Centers for Disease Control, Atlanta, GA, discussed the causes for such a significant decrease (Figure 2). In the US, from 1980 to 2000, approximately 44% of the reduction—equal to more than 150,000 deaths averted—was attributable to changes in risk factors due to behavioral and lifestyle changes, including reductions in total cholesterol (24%), systolic blood pressure (20%), smoking prevalence (12%), and physical inactivity (5%), although these reductions were partially offset by increases in body mass index and the prevalence of diabetes, which accounted for increased numbers of deaths (8% and 10%, respectively). Most of the remainder of the reduction (47% of the total) can be attributed to improved therapies, including secondary preventive therapies after myocardial infarction (MI) or revascularization (11%), initial treatments for acute MI or unstable angina (10%), treatments for heart failure (9%), revascularization for chronic angina (5%), and other therapies (12%) [Ford ES et al. N Engl J Med 2007]. About 9% of the decrease was unexplained.

International Mortality Trends 1968–2003. Men, CHD.
Data indicate that approximately 135,000 lives could have been saved in 2000 by increasing the proportion of eligible patients with CHD who received the appropriate treatment [Capewell S et al. Am J Cardiol 2009]. Important progress has been made since 2000, but their burden, disparities and costs persist and require further risk factor reductions in the future. Strategies that enhance primordial prevention and maximize the delivery of appropriate therapies to all eligible patients with CHD and prioritize medical therapies for secondary prevention and heart failure should be encouraged, as these will be needed as well.
Darwin Labarthe, MD, Centers for Disease Control, Atlanta, GA, summarized the ideals that are driving the Impact 2020 program:
-
to attain high-quality, longer lives that are free of preventable disease, disability, injury, and premature death
-
to achieve health equity, eliminate disparities, and improve health for all
-
to create social and physical environments that promote good health for all
-
to promote quality of life, healthy development, and healthy behaviors across all life stages
These ideals will be achieved through four primary goals:
-
Prevention of risk factors by reducing the proportion of persons in the population with hypertension and the mean total blood cholesterol levels among adults.
-
Detection and treatment of risk factors by increasing the proportion of adults with high blood pressure whose blood pressure is under control and the proportion of persons with CHD who have their low-density lipoprotein cholesterol at or below recommended levels and by reducing the incidence rates for heart disease and stroke.
-
Early identification and treatment of cardiovascular events by increasing the 30-day survival rates following first occurrence of heart disease and stroke.
-
Prevention of recurrent cardiovascular events by reducing the recurrent rates among survivors of heart disease and stroke.
“The overarching objective of the four goals is to increase overall cardiovascular health in the US population,” concluded Dr. Labarthe.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.