

Summary
The metabolic syndrome (MetS) refers to a cluster of metabolic abnormalities that are caused by insulin resistance, which is often associated with intra-abdominal (visceral) obesity, a high-risk form of being overweight/obesity. Cardiometabolic risk encompasses overall cardiovascular disease (CVD) risk that results from traditional risk factors (age, sex, smoking, hypertension, LDL cholesterol, HDL cholesterol, diabetes) and from the additional risks of intra-abdominal obesity and related features of the MetS. Questions remain about the clinical implications of MetS and whether MetS contributes to global CVD risk. These issues were the focus of a special symposium that was organized by the International Chair on Cardiometabolic Risk at the 15th International Symposium on Atherosclerosis 2009 in Boston, Massachusetts, USA.
- Cardiometabolic Disorder
- Obesity
The metabolic syndrome (MetS) refers to a cluster of metabolic abnormalities that are caused by insulin resistance (IR), which is often associated with intra-abdominal (visceral) obesity, a high-risk form of being overweight/obesity. Cardiometabolic risk (CMR) encompasses overall cardiovascular disease (CVD) risk that results from traditional risk factors (age, sex, smoking, hypertension, LDL cholesterol, HDL cholesterol, diabetes) and from the additional risks of intra-abdominal obesity and related features of the MetS. Questions remain about the clinical implications of MetS and whether MetS contributes to global CVD risk. These issues were the focus of a special symposium that was organized by the International Chair on Cardiometabolic Risk at the 15th International Symposium on Atherosclerosis 2009 in Boston.
Neil J. Stone, MD, Northwestern University, Chicago, IL, discussed the concept of MetS and its clinical utility. In the report from the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III, IR was excluded from the MetS criteria due to the degree of difficulty in measuring IR in the clinical setting. However, the ATP III MetS criteria did include five variables that are easily measured in the clinic: waist circumference (WC), triglyceride (TG) levels, HDL cholesterol levels, blood pressure (BP), and fasting glucose levels [NCEP Panel. JAMA 2001]. The presence of defined abnormalities in any three of these five measures constitutes a clinical diagnosis of MetS [Grundy SM et al. Circulation 2005]. Dr. Stone pointed out that metabolic risk should be evaluated after global risk assessment in order to find out if there are metabolic features within that stratum.
Clustering risk factors, such as atherogenic dyslipidemia, elevated BP, elevated blood glucose, proinflammatory state, and procoagulable state, are good signs of the likely presence of MetS. In the Framingham Study, Wilson and colleagues demonstrated that clusters of three or more risk factors were associated with a 2.39 (95% CI, 1.56 to 3.36)- and 5.90 (95% CI, 2.54 to 13.73)-fold greater risk of coronary heart disease in men and women, respectively (p<0.001 for both) [Wilson PW et al. Arch Intern Med 1999]. Additionally, a meta-analysis by Robinson and Stone indicated that metabolic variables greatly enhanced the risk of CVD regardless of LDL cholesterol levels [Robinson JG, Stone NJ. Am J Cardiol 2006]. “Greater metabolic burden means higher cardiovascular risk,” said Dr. Stone.
“Waist circumference is a powerful measure of the underlying pathophysiology,” said Dr. Stone. This concept is the crux of the MetS model. In the INTERHEART study by Yusuf and colleagues, waist-to-hip ratio and WC were closely (p<0.0001) associated with risk of myocardial infarction (MI) worldwide, even after adjustment for other risk factors [Yusuf S et al. Lancet 2005]. MetS diagnosis focuses on the consequences of visceral adiposity, emphasizing lifestyle change and the positive benefit that is associated with increased aerobic activity and moderate weight loss.
Jorge Plutzky, MD, Brigham and Women's Hospital, Boston, MA, discussed additional data that were related to visceral adiposity and MetS. Dr. Plutsky outlined findings that support the concept that fatty acid and gene expression dysregulation may be at the core of MetS. A recent study by Kim and colleagues investigated the effects of overexpression of adiponectin on the metabolic profile of transgenic mice. The transgenic mice demonstrated normalized glucose and insulin levels, as well as reduced serum TG levels. However, they displayed increased expression of PPARγ (the transcriptional regulator of energy balance) target genes and reductions in macrophage infiltration in adipose tissue and systemic inflammation. The transgenic mice were morbidly obese, with significantly higher levels of adipose tissue than their obese (ob/ob) littermates. In this novel model, increased fat mass was associated with improvement in insulin sensitivity [Kim JY et al. J Clin Invest 2007].
Another study, conducted in Dr. Plutzky's lab, investigated the role of endothelial cell PPARγ in metabolism using mice that lacked PPARγ in the endothelium and bone marrow. When these mice were fed a high-fat diet, they had decreased adiposity and increased insulin sensitivity compared with control mice, despite increased serum FFA and TG levels. However, this cohort exhibited significant dyslipidemia and impaired vasoreactivity. They also failed to respond to the FFA- and TG-lowering effects of the PPARγ agonist rosiglitazone. Further bone marrow transplantation studies revealed that these metabolic phenotypes were due to endothelial PPARγ deficiency, suggesting that PPARγ in the endothelium integrates metabolic and vascular responses and that endothelial dysfunction may have a metabolic component [Kanda T et al. J Clin Invest 2009]. Such data may help explain why abnormal endothelial reactivity is among the first changes that are seen in those who are destined for diabetes.
Dr. Plutzky noted that there is still a great deal to learn about fatty acid handling and the role of gene expression in MetS but that we are beginning to observe possible windows into the mechanism of this complex syndrome.
Richard W. Nesto, MD, FACC, FAHA, Lahey Clinic Medical Center, Burlington, MA, discussed the clinical implications of abdominal obesity and MetS, particularly in younger patients. There are currently no specific guidelines for the younger population concerning MetS and CV risk. In a study at Lahey Clinic, consisting of 165 patients who were aged <45 years with acute MI and underwent percutaneous coronary intervention, eight patients had a prior diagnosis of type 2 diabetes mellitus (DM), while an additional 16 patients were diagnosed with type 2 DM at the time of MI or within 3 months of the event. Of the 165 patients, 59% met NCEP criteria for MetS, and obesity was the most common presentation within that group (BMI 32.4±6.3 with MetS vs 27.5±4.5 without MetS; p<0.0001) [Chung EH et al. Am J Cardiol 2007]. “This study is an indication that there has been a background shift in risk factors, particularly in young people, and I suspect that, moving forward, more heart attacks associated with MetS will be seen in this group,” said Dr. Nesto.
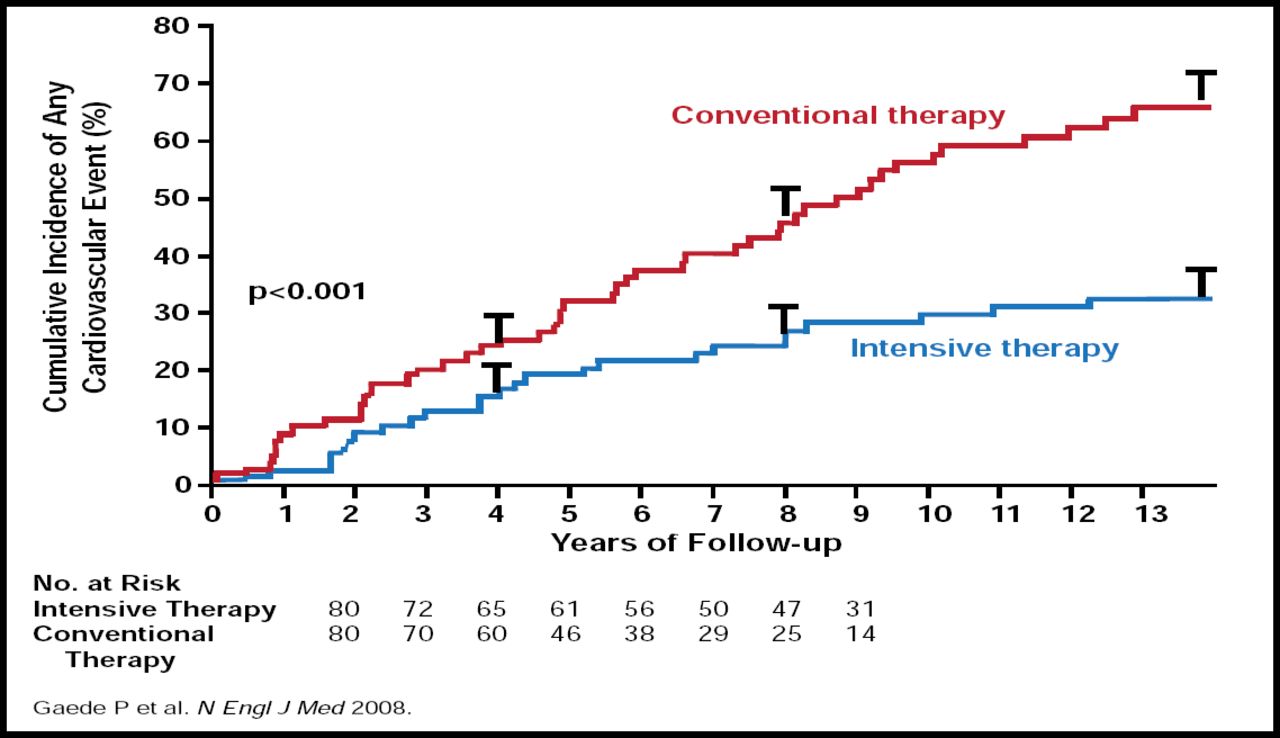
The STENO-2 trial showed significant reduction in CV events with intensive therapy in patients with type 2 DM (p<0.001) [Gaede P et al. N Engl J Med 2008]. Dr. Nesto noted that there was no significant difference in weight loss between the conventional or intensive therapy groups. However, the intensive treatment regimen did involve a prescription for a higher level of aerobic exercise that may have persisted in the follow-up phase (Figure 1).

STENO-2: Reduction in CV Events with Pharmacological Intervention.
Copyright © Massachusetts Medical Society 2008. All rights reserved.
Obesity is an insulin-resistant, proinflammatory, and prothrombotic state that interacts with risk factors to accelerate atherosclerosis and cardiac muscle disease. Dr. Nesto emphasized the need to regard obesity as a major risk factor for CVD and type 2 DM. Early lifestyle intervention to prevent abnormalities in cardiac structure and function may be the key to better outcomes.
H. Bryan Brewer Jr, MD, MedStar Research Institute, Washington, DC, discussed the global issue of MetS and the importance of differentiating between the “healthy obese” and those with MetS. Identification of patients with visceral adiposity and dyslipidemia, particularly elevated TGs, is a good indicator of MetS versus the “healthy obese.” Weight reduction is important, but the question remains whether or not we can change the dynamic of the MetS in young patients with simple weight reduction.
Dr. Brewer added that lipoprotein profile is important and that focus should not be limited to LDL. The VA-HIT study tracked coronary events that were related to the presence and absence of IR with lower and higher levels of HDL and TGs. This study demonstrated that the occurrence of a new CV event and the benefit of fibrate therapy were much less dependent on levels of HDL cholesterol or TGs than on the presence or absence of IR [Robbins SJ et al. Diabetes Care 2003]. Additional studies have shown that the combination of statins and fibrates provided more effective control of multiple lipid parameters than monotherapy alone in patients with mixed dyslipidemia [Mohiuddin SM et al. Am Heart J 2009]. Weight reduction and treatment of dyslipoproteinemia are crucial in the clinical management of global CMR, concluded Dr. Brewer.
Dr. Després concluded the session by emphasizing that the mosaic of modifiable CVD risk factors has evolved over the last few decades. Indeed, the key drivers of CVD risk in the post-Second World War period were smoking, undiagnosed hypertension, and hypercholesterolemia. Now, the epidemics of obesity, MetS, and type 2 DM represent a challenge in our ability to successfully fight CVD worldwide.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.