

Summary
Some of the results from the Systematic Enhancement Treatment Program for Bipolar Disorder [STEP-BD] trial are presented in this article. The primary focus of STEP-BD was to determine whether or not standard antidepressants are effective treatment for bipolar disorder [N Engl J Med 2007].
- mood disorders
- psychopharmacology
Some of the results from the Systematic Enhancement Treatment Program for Bipolar Disorder (STEP-BD) were presented by Gary Sachs, MD, Harvard Medical School, Boston, MA. The primary focus of STEP-BD was to determine whether or not standard antidepressants are effective treatment for bipolar disorder [N Engl J Med 2007], and as the study was being designed, Dr. Sachs had expectations regarding the outcome. “I had gone my entire career believing that these drugs were not so effective and, in fact, that they often caused worsening. And here I was putting together a study to convince myself I might be wrong.”
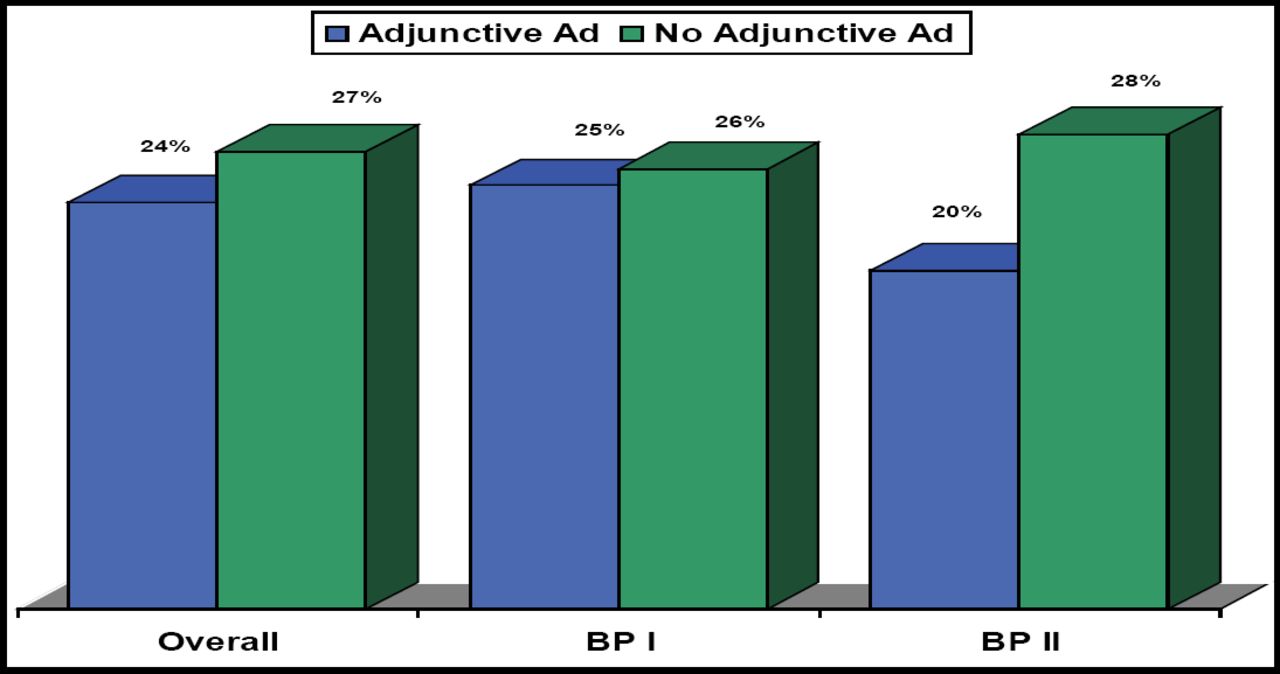
In this double-blind, placebo-controlled study, Dr. Sachs randomized 366 patients with bipolar depression to receive up to 26 weeks of treatment with mood stabilizers and either adjunctive antidepressant or matching placebo. Choice of mood stabilizer (MS) was lithium or valproate; the antidepressants (AD) that were used were paroxetine or bupropion. Study endpoints were durable recovery, defined as ≥8 consecutive weeks euthymic; transient remission, being euthymic 1 to 7 weeks; effectiveness response, a 50% improvement from baseline depression scores; or nonresponder.
Durable recovery was 23.5% with antidepressant adjunctive treatment, as compared with 27.3% recovery for patients who received no additional medication (Figure 1). Effectiveness response was 32.4% versus 38.0%, and transient remission was 41% versus 49% for MS/AD versus MS, respectively (for all results, p>0.23).

Proportion Achieving Durable Remission.
Dr. Sachs then went on to analyze results for treatment-emergent affective switch, mindful that he often had seen patients switch when antidepressants were added to the mix. However, results contradicted his expectations. “Now, this is something I've believed my entire career, and we actually selected paroxetine and bupropion because they are historically less associated with switch.” No difference was noted between the treatment arms (10.1% vs 10.7%).
Another pilot study to emerge from STEP-BD looked at the addition of lamotrigine, inositol, or risperidone to antidepressants (n=66; Nierenberg. Am J Psychiatry 2006). All patients were in a current major depressive episode that was nonresponsive to a combination of adequate doses of established mood stabilizers plus at least one antidepressant. Results for durable recovery in this setting were: risperidone 5%; inositol 17%; and lamotrigine 24%. “So, maybe we have something here with inositol or lamotrigine,” said Dr. Sachs, “but risperidone does not look like something to further explore.”
What about psychiatric interventions? Dr. Sachs reviewed one study—an extension of the investigation described above—that used psychosocial intervention in addition to protocol pharmacotherapy (n=293; Miklowitz D. Arch Gen Psychiatry 2007). Patients were randomly assigned to intensive psychotherapy or collaborative care (a brief psycho-educational intervention). Results showed that patients who received intensive psychotherapy had significantly higher year-end recovery rates (64.4% vs 51.5%) and shorter times to recovery than patients in collaborative care (p=0.01). “The big news is, when they got better, they got better on average 110 days sooner. For most of our patients, that is a clinically meaningful difference.”
Dr. Sachs did point out a caveat to this presumed good news. In a similar trial of 253 depressed bipolar patients who were treated with medication and cognitive behavioral therapy (CBT), it was determined that overall there was no benefit of adding CBT to treatment as usual. Adjunctive psychotherapy was beneficial in patients who had 1 to 6 prior episodes but was inferior to medication alone for those patients who had had more than 30 previous episodes. “Earlier in the course of disease appears to be when these interventions are most likely to be the most beneficial.” Dr. Sachs considered these results to be analogous to the rehabilitation of a heart patient—those who had one or few cardiac events might be expected to fully recover, but those patients who had repeated events might be best advised to avoid intensive exercise.
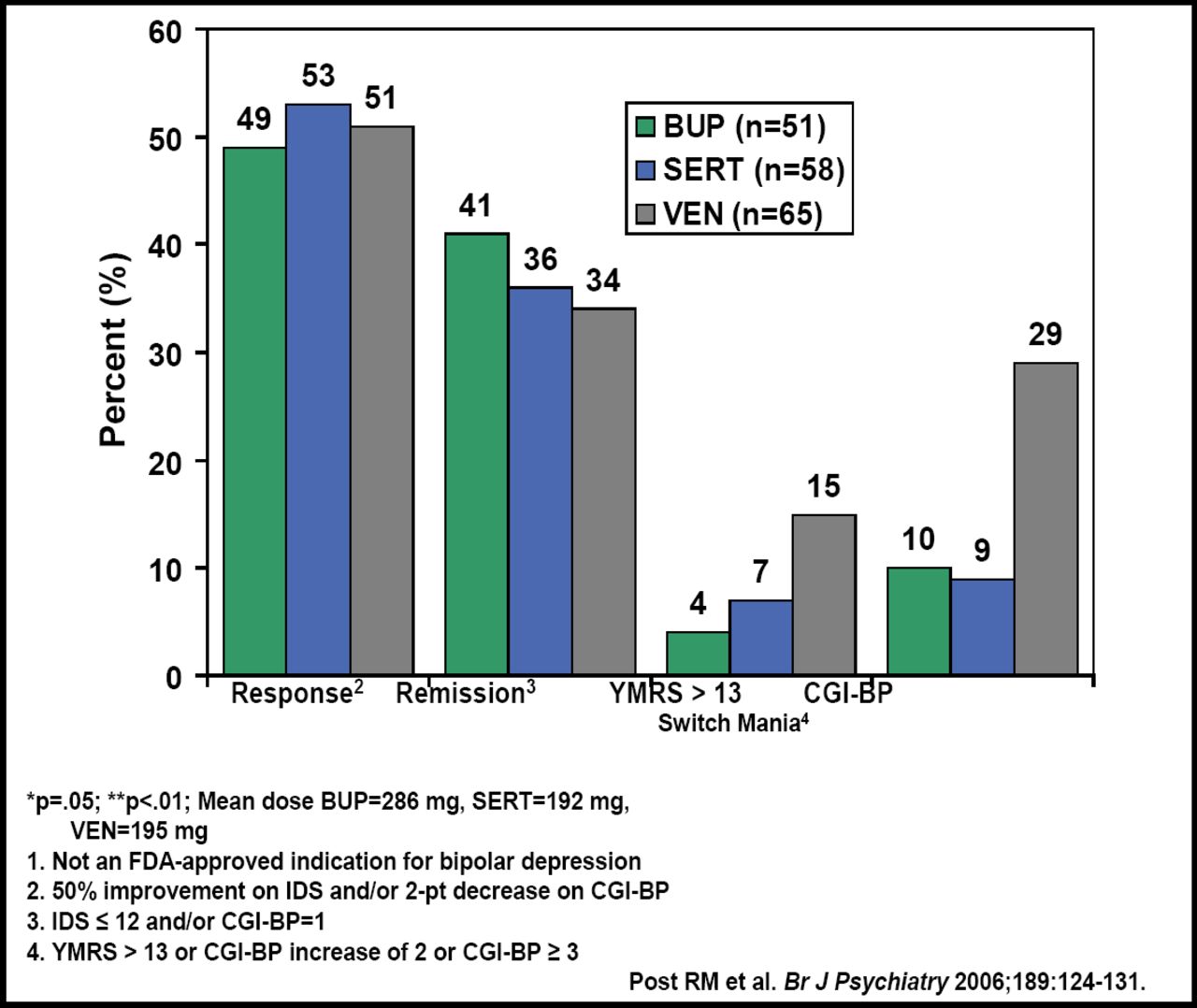
Mark Frye, MD, Mayo Clinic Mood and Research Program, Rochester, MN, presented more encouraging results for the treatment of bipolar depression with antidepressants [Post RM. Br J Psychiatry 2006]. “We use these medicines all the time and we need to know if they work, and if they do, for what patient population. Secondly, we need to know that they are safe.” The study was a 10-week, multicenter, randomized double-blind investigation of adjunctive treatment with either sertraline (50–200 mg/day), bupropion (75–450 mg/day) venlafaxine (37.5–375 mg/day), or matching placebo. All patients received mood stabilizers (n=174). Patients had inventory depression symptomatology (IDS) ≥16 and CGI ≥3. Patients who had a YMRS ≥14 or a CGI-BP mania severity of ≥3 at baseline were excluded. Endpoints for response were ≥50% improvement in IDS, ≥2 point decrease in CGI-BP depression score; remission was defined as IDS <12 or CGI-BP score of 1; and switch, a 2-point increase at any point on the CGI-BP mania severity scale.
Results showed that all 3 antidepressants were associated with a similar range of acute response (49% to 53%), which answered Dr. Frye's first question regarding whether or not antidepressants work in this setting. “In contrast to the STEP data, we found that almost half of our cohort bipolar patients who were on mood stabilizers responded to adjuvant antidepressant therapy. We saw no difference by drug in regard to response or remission rate.” Recall that his second question addressed safety: In fact, differences did emerge for incidence of switching. “When we looked at destabilizing elements, we did see a difference, suggesting that switch rates were higher with venlafaxine,” defined by either YMRS or CGI-BP scales (p<0.05; Figure 2).

Antidepressant Response and Remission.
In a sub-analysis of the switch data, non-rapid cycling patients were found to have equivalent switch rates between treatment arms; amongst rapid cyclers, however, those who were treated with bupropion had significantly lower rates for switching as compared with those patients who were treated with venlafaxine (p<0.01). There were no differences that were observed in this analysis for bupropion versus sertraline, or sertraline versus venlafaxine. The majority of those patients who switched was bipolar I. “That struck us as odd because the bipolar I's were the most aggressively controlled with mood stabilizers.” Upon further examination, switching subjects were found to have minimal manic symptoms in syndromal depression at baseline—minimal, as in YMRS scores <4—yet higher symptoms than those patients who didn't switch.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.