

Summary
It is estimated that 25–45% of patients with schizophrenia do not respond to treatment. Treatment resistant patients have typically been defined as those that have failed two adequate courses of two different neuroleptic drugs. This article discusses high dose atypical antipsychotics in these patients, as well as brain morphology in schizophrenia, and treatment algorithms for obsessive compulsive disorder with schizophrenia.
- Schizophrenia
- Anxiety Disorders
High Dose Atypicals for Refractory Schizophrenia: Approach with Caution
It is estimated that 25–45% of patients with schizophrenia do not respond to treatment, a statistic that was reflected by the large number of attendees at an APA session regarding treatment strategies in these patients. Treatment resistant patients have typically been defined as those that have failed two adequate courses of two different neuroleptic drugs. Jean-Pierre Lindenmayer, MD, New York University Medical Center, led a session on high dose atypical antipsychotics in these patients.
Dr. Lindenmayer prefers to define treatment resistance by looking at individual symptoms to determine the areas in which patient is refractory (eg, positive symptoms, negative symptoms, cognitive symptoms, excitement/assaultiveness/violence, and anxiety/depression/suicide). He then presented a plan to determine whether a therapy is working for a patient, and if not, how to proceed. The first step is to review the diagnosis, ruling out possible psychiatric and medical comorbidities. Prior pharmacotherapy should also be evaluated to verify that the medication dose was appropriate, the patient was compliant, and the drug was taken long enough to produce an effect. “It is not always easy, as many of you probably know, to get an accurate record of what your patient has been on, what he has responded to, and how long these different trials were done,” commented Dr. Lindenmayer. Plasma levels of current medications should also be assessed. If a patient is indeed refractory, the areas of non-response should be elucidated, a sequential treatment plan should be developed, and a rating instrument such as the Clinical Global Impressions, Brief Psychiatric Rating Scale, or the Positive and Negative Syndrome Scale should be utilized to measure progress.
Increasing doses of atypical antipsychotics is one obvious approach to treating refractory patients. A review of patient data from the New York State psychiatric system found that many patients receive medication at doses higher than what is approved by the FDA (Table 1). Such an approach, however, is not without risks. In addition to the extra costs, patients may experience increased side effects, and there is a lack of controlled data with these higher doses. Data from several studies of higher dose atypicals in patients with schizophrenia was presented (Table 2). “If high dose therapy is considered, good documentation and patient information are absolutely essential. You certainly would want to monitor patients closely with accurate laboratory data and periodic review in terms of where they stand more frequently than if you stayed within the FDA-approved dose,” concluded Dr. Lindenmayer.
Percentage of Patients Receiving Higher than FDA-Approved Doses in the New York State Psychiatric System.
Review of High Dose Atypical Antipsychotics in Schizophrenia.
Northern Finland 1966 Birth Cohort: Brain Morphology in Schizophrenia
The Northern Finland 1966 Birth Cohort is a large sample of pregnant women that were due to give birth in 1966, resulting in 12,058 live births. Medical, environmental, and social data were collected prior to birth and longitudinally over the last 41 years. This cohort has offered a unique opportunity to study individuals with schizophrenia, and Matti Isohanni, MD, University of Oulu, Finland, presented preliminary results regarding brain morphology in patients diagnosed with schizophrenia. A total of 157 subjects had a psychotic episode prior to age 31. Of these, 110 (70%) had a DSM-III R diagnosis of schizophrenia, and the remaining 47 (30%) had other psychoses. At approximately age 34 years, 54 subjects with schizophrenia and 100 randomly selected control subjects were assessed with structural MRIs. Specifically, the investigators sought to determine how morphologic abnormalities related to symptom severity and duration of illness. Significantly different areas of the brain between the two groups of patients were identified through the use of computational morphometry and non-parametric statistics. Symptom severity was measured using the Positive and Negative Syndrome Scale (PANSS), the Clinical Global Impression (CGI) scale, and the Social and Occupational Functional Assessment (SOFA).
When looking at the brain as a whole, there were no significant differences between the groups with respect to white matter, gray matter, or cerebrospinal fluid. However, regional differences in grey matter were identified. In patients with schizophrenia, bilateral gray matter deficits were evident in the brain stem, cerebellum, basal ganglia, cingulate, precuneus, cuneus, insula, fusiform gyrus, superior, inferior and middle frontal gyrus, superior and medial temporal lobe, and the central gyri (7% decrease vs controls; p<0.001). Conversely, patients with schizophrenia had an excess of gray matter in bilateral medial frontal gyrus, cingulate, basal ganglia, parahippocampal gyrus, and insula (10% greater than controls; p<0.00001). Gray matter areas that were considered significantly different between the two groups were linked to symptom severity and the duration of illness. The loss of regional gray matter generally had significant associations with cognitive functioning, CGI scores, and SOFA scores, and a strong association with duration of illness (p<0.001). “The longer the duration of illness, the less gray matter in these critical areas,” commented Dr. Isohanni. This suggests that the illness is progressive, but the variability in age at onset of symptoms may potentially confound the data. Cohort members will undergo their mid-life assessments in 2007–2010.
Treatment Algorithm for Obsessive Compulsive Disorder with Schizophrenia
Michael Hwang, MD, Wilkes Barre Pennsylvania VA Hospital, gave an overview of comorbid obsessive compulsive disorder (OCD) in patients with schizophrenia. Prevalence estimates for schizophrenia with OCD have increased over time, from a report of 1.1% in 1926 to 26% in 2003. It is possible that the advent of approved medications for the treatment of OCD may have influenced the recognition of comorbid OCD in schizophrenia, causing its prevalence to rise. Several hypotheses have emerged regarding these two disorders: 1) that this is schizophrenia with comorbid OCD, 2) this is schizophrenia with OC dimensions, and 3) it is a subtype of schizophrenia.
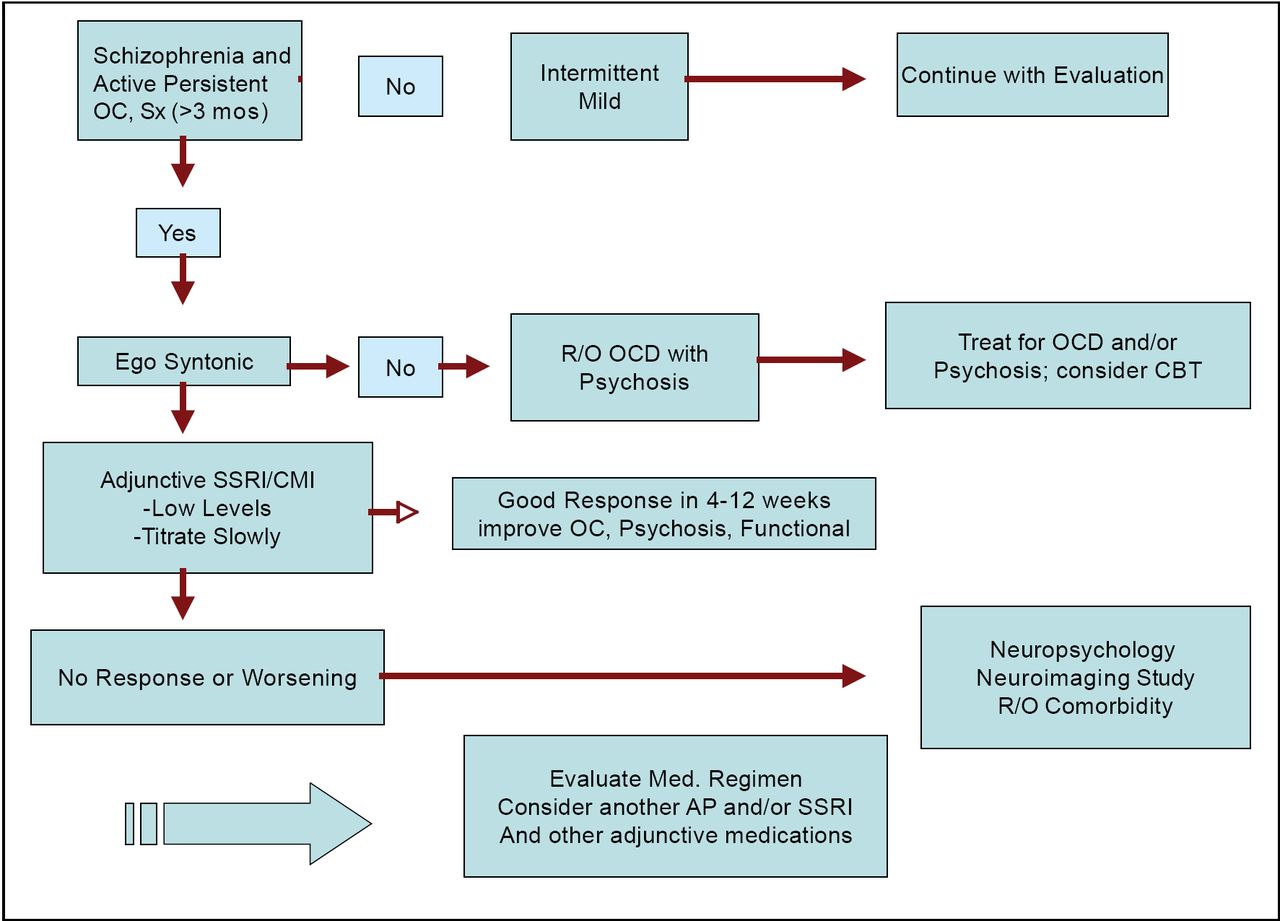
“How do you treat these patients? I think the schizophrenia patients with OC symptoms are quite diverse in their phenomenology and the underlying pathogenesis. It is important to assess the full symptom picture of the patient and identify all associated symptoms,” said Dr. Hwang. An algorithm for the clinical management of these patients was presented (Figure 1).
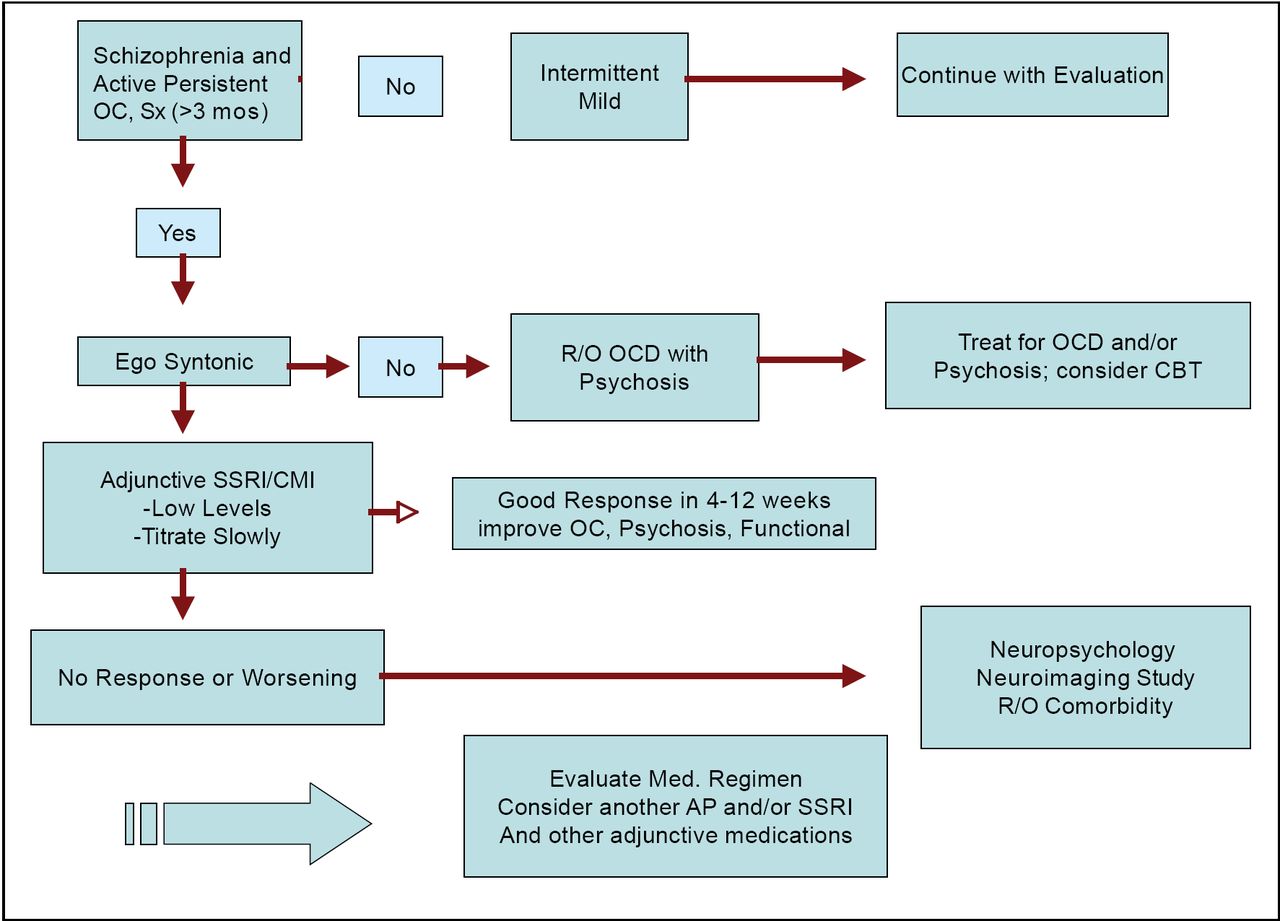
Treatment of Obsessive Compulsive Schizophrenia.
“Generally a literature review will indicate that the atypical antipsychotic medication will worsen OC symptoms,” commented Dr. Hwang, but he emphasized that this may not always be the case, since individual responses to medications will be highly variable. If treatment with adjunctive SSRIs is initiated, they should be started at a low dose and titrated very slowly. “I think many of us, myself included, have failed when we titrate the dose too rapidly,” summarized Dr. Hwang.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.