

Summary
This article discusses the effect of trastuzumab on cardiac function, the final results from the phase 3 Intergroup Trial E1199, novel regimens for the treatment of triple-negative breast cancer tumors, and a comparison of magnetic resonance imaging versus mammography in detecting ductal carcinoma in situ.
- Adjuvant/Neoadjuvant Therapy
- Breast Cancer
- Radiology
The incidence of congestive heart failure (CHF) associated with trastuzumab, for early breast cancer treatment, does not increase over time, according to a 5-year update of cardiac dysfunction in patients in the adjuvant NSABP B31 trial.
While CHF occurred more often in patients who received trastuzumab, versus those who did not, the cumulative incidence at 5 years was no greater than the incidence observed at 3 years, reported Priya Rastogi, MD, University of Pittsburgh Cancer Institute.
NSABP B31 compared adjuvant doxorubicin/cyclophosphamide followed by paclitaxel, to the same regimen plus trastuzumab for 1 year. The initiation of trastuzumab required normal post-AC left ventricular ejection fraction (LVEF) on MUGA scan. Nearly 8% of women did not receive trastuzumab on the basis of positive cardiac findings.
The 1,850 women who were randomized to standard treatment or treatment plus 1 year of trastuzumab were carefully followed for cardiac toxicity with periodic MUGA scans. If symptoms suggestive of CHF developed, the records were blindly reviewed by a panel of cardiologists to determine whether criteria were met for a cardiac event, defined as NYHA class III or IV CHF or possible/probable cardiac death.
After 5 years, the cumulative incidence of cardiac events was 0.9% with standard treatment and 3.8% when trastuzumab was added for 1 year (Table 1). The incidence was similar to that reported at 3 years, and most patients on trastuzumab recovered full cardiac function, Dr. Rastogi reported.
5 Year Cumulative Incidence of Cardiac Events in the Evaluable Cohorts.
Arm 1: AC→PTX, n=898, 6 CHFs, 1 Cardiac Death
Arm 2: AC→PTX + Trastuzumab, n=947, 35 CHFs, No Cardiac Deaths
“We are encouraged by these new data showing no additional late cardiotoxicity associated with trastuzumab,” she said.
Of 33 trastuzumab patients in whom a cardiac event was confirmed, 5 were symptomatic in the 6 months prior to the ASCO presentation, and 20 were still on medication (Table 2). While ejection fractions tended to normalize by 18 months, they remained above baseline levels in some patients, she added.
As part of the study, investigators examined potential risk factors for cardiac toxicity and identified advanced age (>65), use of hypertension medications at baseline, and low baseline ejection fraction as important. Radiation site was not a significant predictor.
Recovery of Patients Reporting Symptoms of Possible CHF.
By individual risk factor, the incidence of heart failure was 5.4% for patients >65 compared to 2.3% for those <50 years of age; 6.8% for patients on antihypertensives vs 3% for others; and 12.9% for patients with baseline ejection fraction <54%, compared to 2.1% when ejection fraction was >65 (Table 3), Dr. Rastogi reported.
Risk Factors for Cardiac Toxicity.
A prediction model incorporating these risk factors was able to show, for example, that cardiac risk was only 1.3% for a 48-year-old female with a baseline ejection fraction of 69% who was not on antihypertensive medication, but rose to 15% in a 57-year-old patient with an ejection fraction of 54% who was on a blood-pressure-lowering agent.
Dr. Rastogi advised clinicians to consider individual risk for cardiac events when deciding whether to administer trastuzumab.
Taxanes Comparable in Adjuvant Regimen
In adjuvant regimens for early breast cancer, the choice of taxane—docetaxel or paclitaxel—may be unimportant, in terms of disease-free survival, according to the final results from the phase 3 Intergroup Trial E1199, reported by Joseph Sparano, MD, Albert Einstein College of Medicine, New York.
Evidence has suggested that docetaxel is more effective than paclitaxel, and paclitaxel is more effective when given weekly versus every 3 weeks in metastatic breast cancer. This study evaluated these agents and schedules in the adjuvant setting.
E1199 randomized 4,590 patients with node-positive or high-risk node-negative breast cancer to doxorubin 60 mg/m2 plus cyclophosphamide 600 mg/m2 (AC) every 3 weeks for 4 cycles, followed by either (1) paclitaxel 175 mg/m2 every 3 weeks for 4 cycles, (2) paclitaxel 80 mg/m2 weekly for 12 cycles, (3) docetaxel 100 mg/m2 every 3 weeks for 4 cycles, or (4) docetaxel 35 mg/m2 weekly for 12 cycles. The primary comparisons included taxane (docetaxel vs paclitaxel) and schedule (weekly vs every 3 weeks).
At a median follow-up time of 64 months, no differences in disease-free survival (DFS) were shown. There was, however, a 5% absolute improvement in DFS with paclitaxel given weekly and with docetaxel given every 3 weeks, and a 3% absolute improvement in overall survival with paclitaxel given weekly, Dr. Sparano reported.
“Compared with paclitaxel, docetaxel did not improve disease-free survival. And compared with a regimen given every 3 weeks, weekly treatment did not improve disease-free survival,” he said, referring to the primary endpoints (Table 1).
Outcomes by Taxane and Regimen.
With weekly paclitaxel and q-3-week docetaxel, the risk of disease progression was reduced by 25%. Similar trends observed in hormone-receptor-negative and hormone-receptor-positive patients. Weekly paclitaxel improved overall survival, reducing the risk of death by 30% over other arms.
Toxicity was generally mild, with some differences between the regimens. The q-3-week docetaxel arm was associated with more severe neutropenia, febrile neutropenia, and infection, while weekly paclitaxel was associated with more neuropathy. The neuropathy with paclitaxel was reversible in most patients, he added.
As the discussant for this presentation, Robert Carlson, MD, Stanford University Palo Alto, California, concluded, “Weekly paclitaxel is substantially more effective than paclitaxel given every 3 weeks, and weekly paclitaxel is more effective than either docetaxel regimen. The toxicity profile also favors weekly paclitaxel.”
Triple-Negative Breast Cancer Tumors Have Good Response to Novel Regimen
In the adjuvant treatment of breast cancer, a regimen of anthracycline plus paclitaxel (without cyclophosphamide) followed by weekly paclitaxel (AP→wP) may be as effective as the standard regimen of anthracycline/cyclophosphamide (AC) followed by paclitaxel given every 3 weeks (AC→P). The study was reported by David Loesch, MD, of US Oncology, Houston, Texas.
“Anthracycline/paclitaxel followed by weekly paclitaxel can be considered a standard treatment in the community,” Dr. Loesch said, “although it is more neurotoxic and must be used with caution.”
In particular, this regimen was of the greatest benefit in the patients with “triple-negative” breast cancer: HER2-negative, estrogen receptor (ER)-negative, and progesterone receptor (PR)-negative, he reported. Especially in these patients, AP→wP was superior to AC→P, he reported.
The study randomized 1,830 early breast cancer patients to one of these arms. About two thirds of each arm were ER+ and/or PR+, while one third were negative for hormone receptors. About two thirds were also HER2-negative. Most patients had 1–3 positive lymph nodes.
In a previous interim analysis, disease-free survival at 3 years was significantly better with AP→wP: 88% vs 85% with AC→P, for a 26% reduction in relapse (p=0.05). However, the current 5-year analysis found no difference between the arms: 81% vs 80% (p=0.38), Dr. Loesch reported.
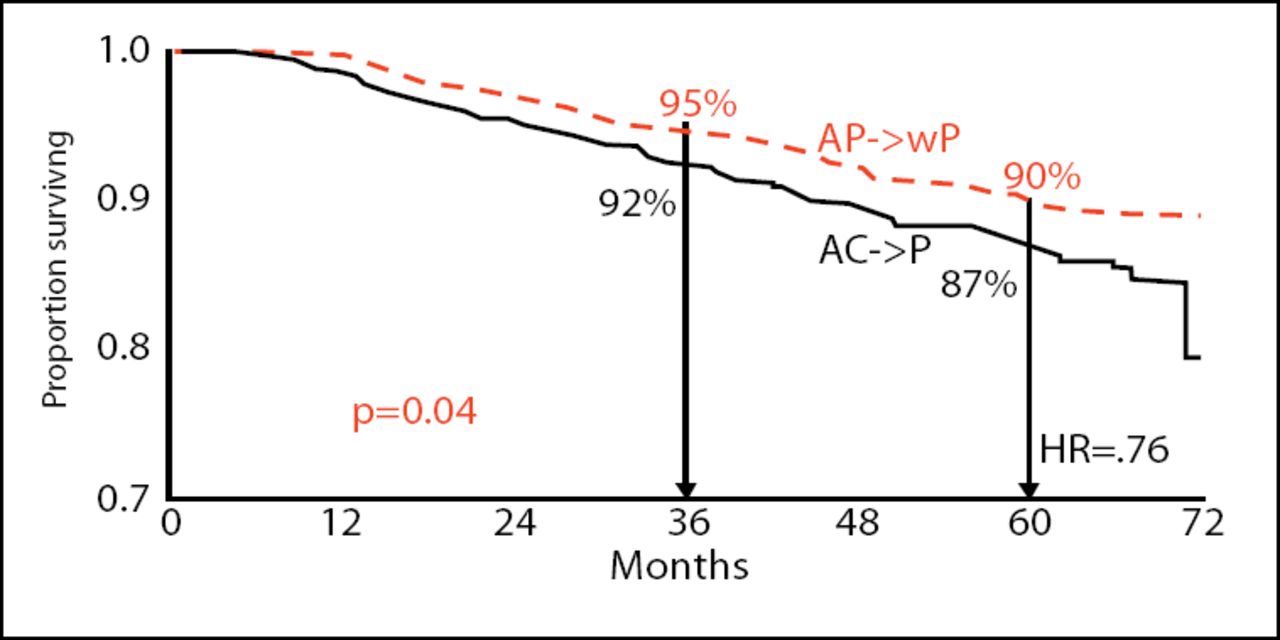
However, the differences in overall survival that were previously reported were maintained in the ASCO report. At 5 years, overall survival was 90% with AP→wP compared with 87% with AC→P, for a 24% reduction in risk with AP→wP (p=0.04; Figure 1).
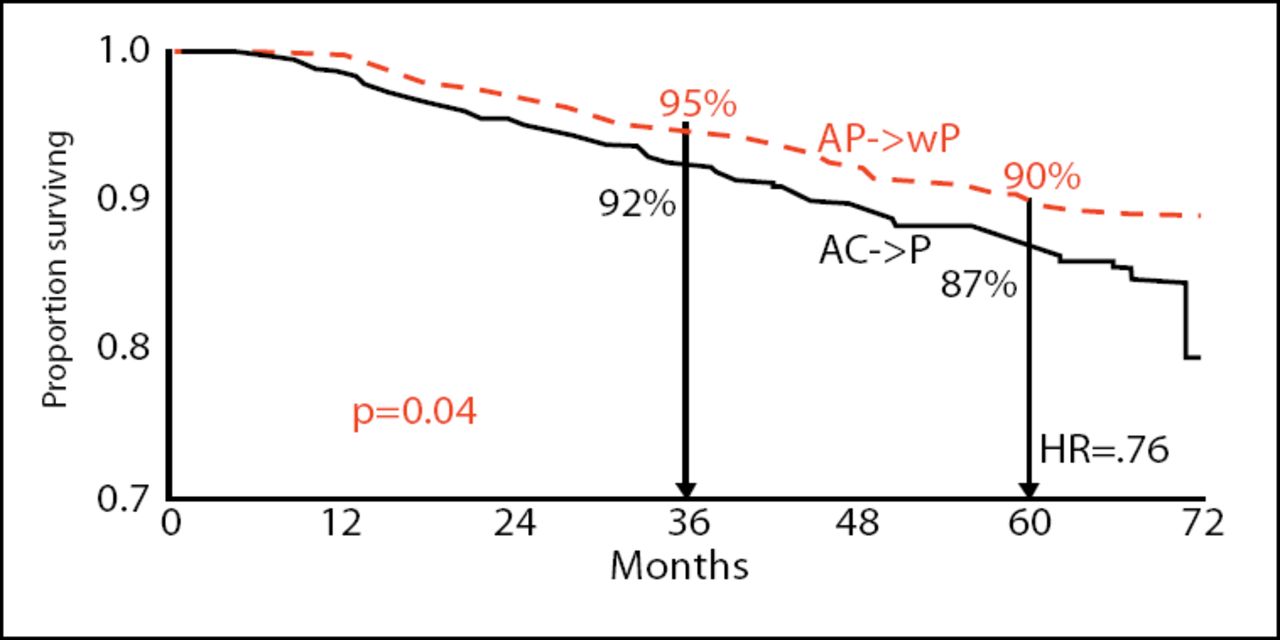
Overall Survival (ITT).
This 3% absolute survival difference was based on the considerable number of deaths in the AC→P arm: 106 vs 80 for AP→wP. Breast cancer deaths numbered 83 and 63, respectively.
“Omitting cyclophosphamide in the AP→wP regimen did not compromise disease-free survival or overall survival,” he pointed out.
There were no differences in disease-free or overall survival between the arm based on hormone receptor status or HER2 status. But in the unplanned analysis of triple-negative tumors, AP→wP was clearly superior. In fact, the superiority in this arm probably accounted for the difference in overall survival that was seen, according to the investigators.
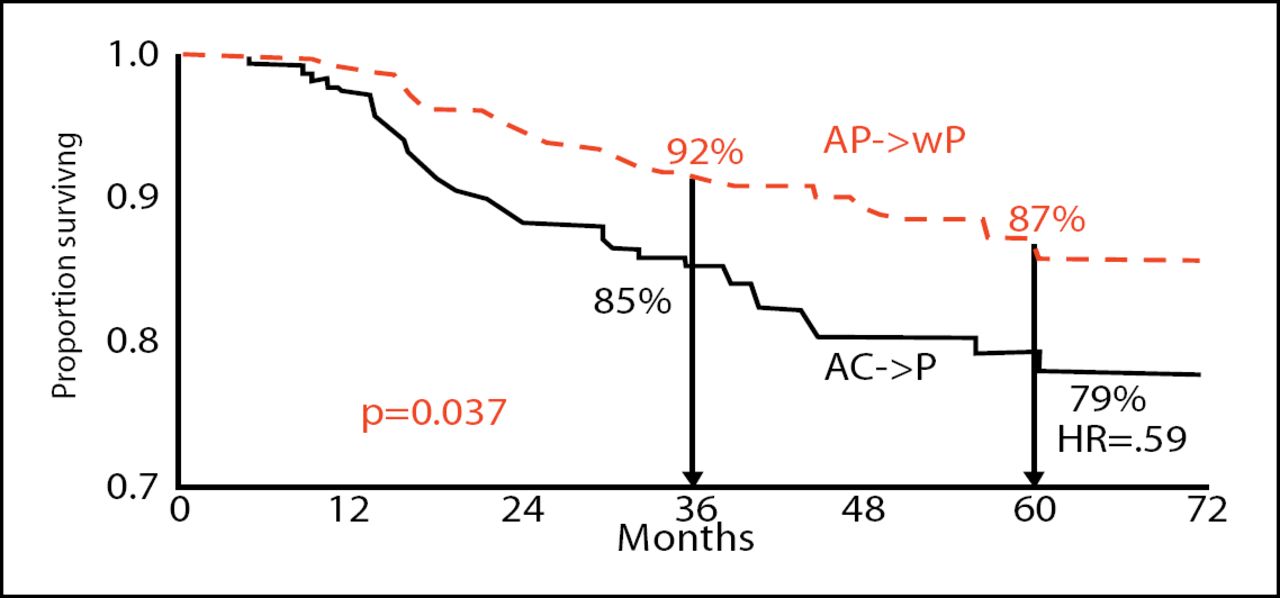
Among the 378 triple-negative patients, disease-free survival at 5 years was 79% for the AP→wP arm and 74% for the AC→P arm, for a 41% reduction in risk. Overall survival was 87% and 79%, respectively. Again, this represented a 61% reduction in risk in this subgroup (p=0.037; Figure 2), Dr. Loesch reported.
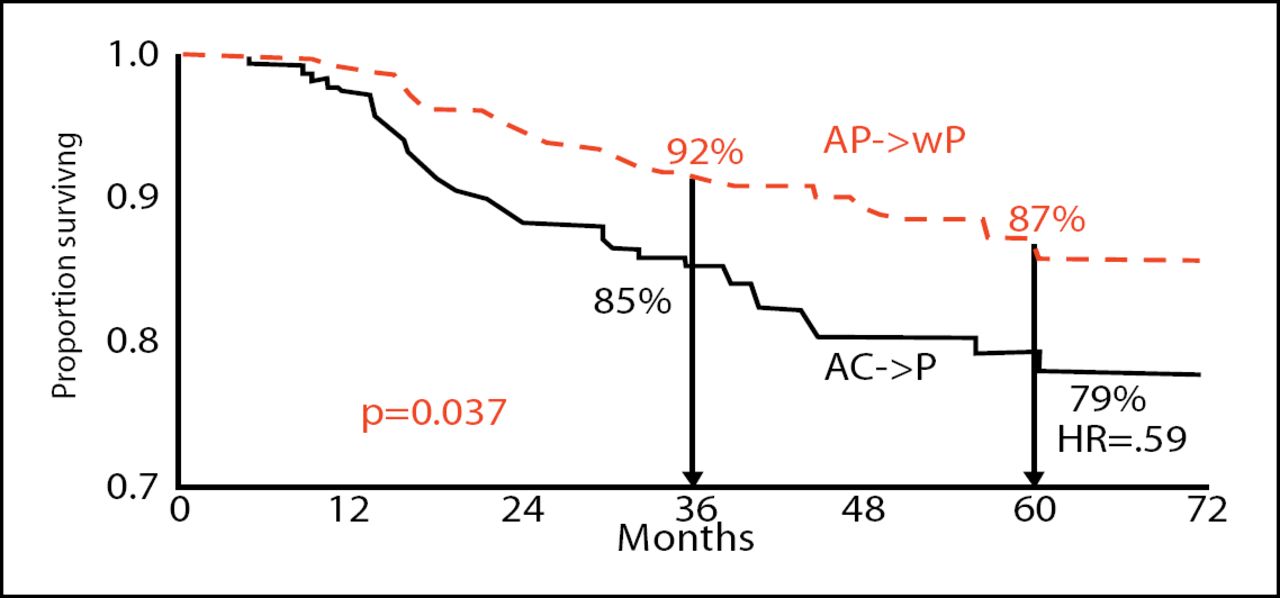
Overall Survival for Triple Negative ER-/PR-/HER2neu.
There was no difference in cardiotoxicity between the arms. Nonhematologic toxicity was primarily neuropathy, which was 32% with the AP→wP regimen and 17% with AC→P (p<0.01).
The study's discussant, Robert Carlson, MD, Stanford University, Palo Alto, California, noted the better outcomes with AP→wP in the triple-negative patients. But he said that, in his opinion, the study “does not change practice in early disease or in the triple-negative subset.”
MRI More Accurate than Mammography in Diagnosing Aggressive DCIS
In a breast cancer screening population, magnetic resonance imaging (MRI) was more effective than mammography in detecting ductal carcinoma in situ (DCIS), especially high-grade lesions that are most likely to progress, a recent German study found.
Cristiane K. Kuhl, MD, University of Bonn, Germany, noted that mammography is the standard means of diagnosing DCIS but often results in the over diagnosis of low-grade lesions that are not clinically meaningful. MRI has recently become established as superior in the diagnosis of invasive breast cancer in high-risk women, but is still controversial in the case of DCIS, she said. The study investigators aimed, therefore, to clarify the value of MRI in diagnosing DCIS that is clinically important.
The prospective study included 5,960 women referred to a dedicated breast unit for screening or for diagnostic assessment (ie, an unselected cohort). Women underwent bilateral mammography with at least two views, plus spot compression views where appropriate, and high-resolution bilateral MRI.
A total of 167 women received the final pathologic diagnosis of DCIS. This included 44 low-grade lesions, 34 intermediate-grade lesions, and 89 high-grade lesions. Of these women, 89% had been referred for regular screening, 10% for high-risk screening, 7% for follow-up after breast cancer, and 4% for clinical symptoms. Women were assessed for mode of detection and the biologic profile of the DCIS (size, nuclear grading, hormone receptor status and HER2/neu status).
Of the 167 DCIS cases, the diagnosis was made only on MRI in 153/197 (92%), and only by mammography in 93/167 (56%), Dr. Kuhl reported.
MRI was significantly more sensitive for all lesion grades, and was substantially more sensitive in diagnosing high-grade lesions. Among cases diagnosed by MRI, 69% were high-grade lesion; among the mammography-diagnosed cases, 17% were high-grade. MRI-detected lesions were also more likely to estrogen-receptor-negative and HER2-positive, compared to mammography-diagnosed lesions, she said.
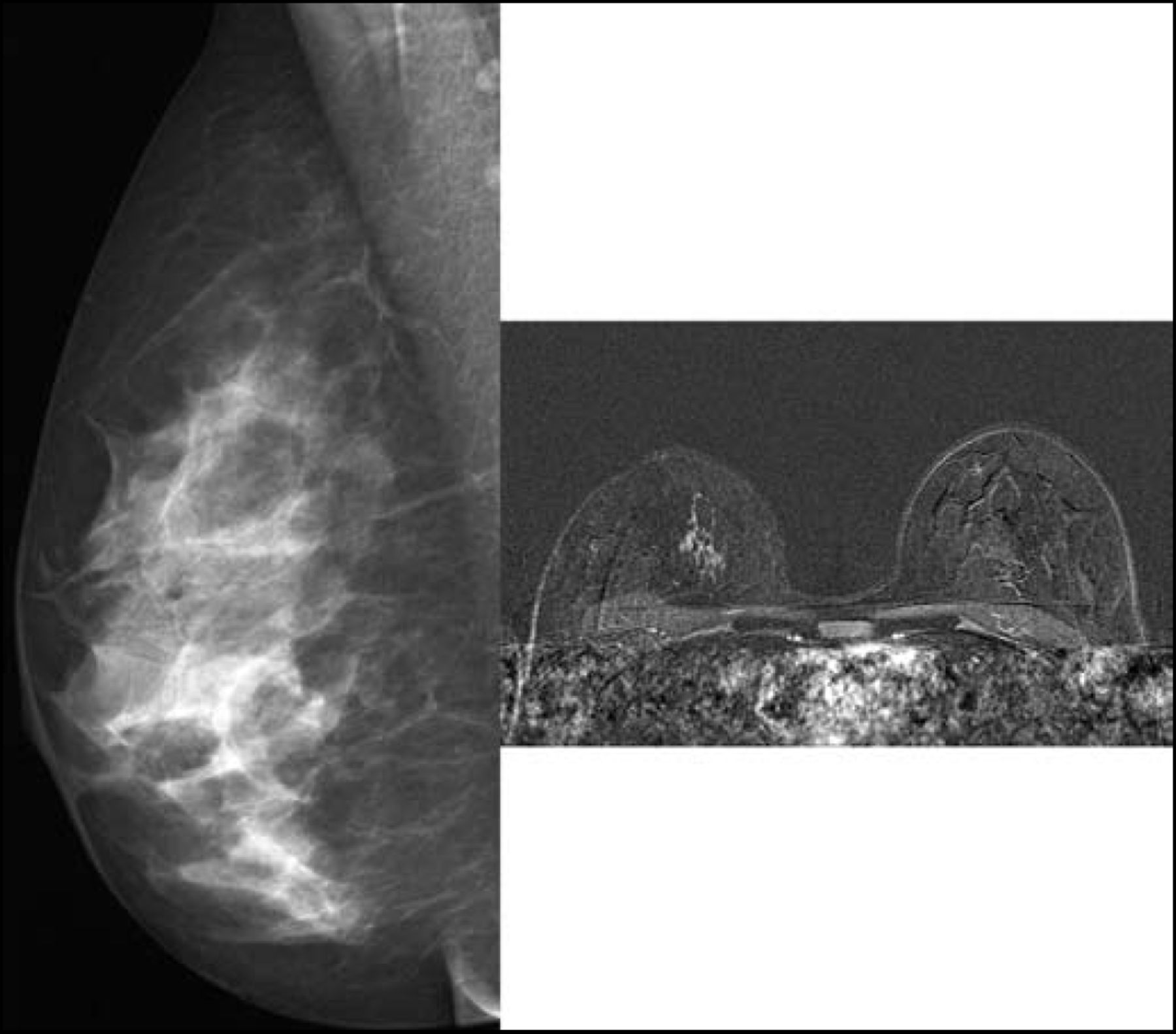
Digital Mammogram of a patient with High Grade DCIS (Read as Normal) (left).
MRI Study of a Patient with DCIS in the Upper Inner Quadrant of Right Breast (right).
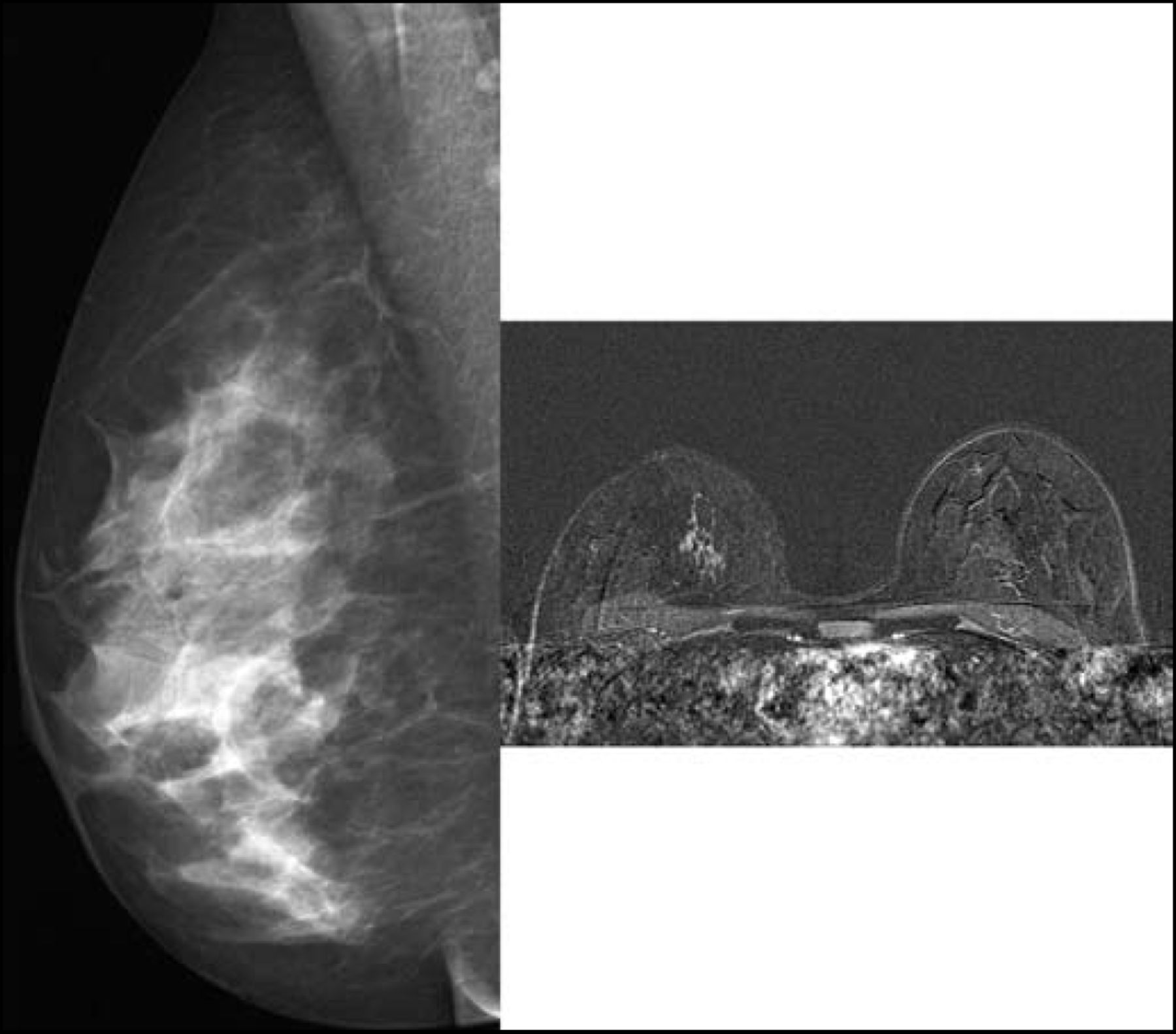
Images courtesy of Cristiane K. Kuhl, MD, University of Bonn
There were no differences between the lesions detected by MRI versus mammography in terms of patient age, history of breast cancer, familial risk, breast density, or menopausal status.
“MRI was more sensitive than mammography for diagnosing DCIS, and particularly high-grade lesions. Over half of all high-grade lesions were diagnosed only by MRI,” Dr. Kuhl concluded. “MRI detects DCIS with an aggressive biological profile.”
“It is important to diagnose high-grade DCIS for breast cancer prevention. This is another piece of evidence that MRI is the new gold standard, adding to information that it is better for detecting invasive cancer in high-risk patients,” she said. While MRI was more sensitive in this study, the impact of MRI on long-term outcomes, however, remains unknown.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.