

Summary
This article presents an overview of some of the work that has been done to identify prognostic indicators for progression of hip and knee arthritis and about the markers of osteoarthritis (OA). Other topics discussed include an analysis of the GARP Study, radiographic views and scoring methods available to identify structural damage in knee OA, and the future of OA treatment.
- arthritis
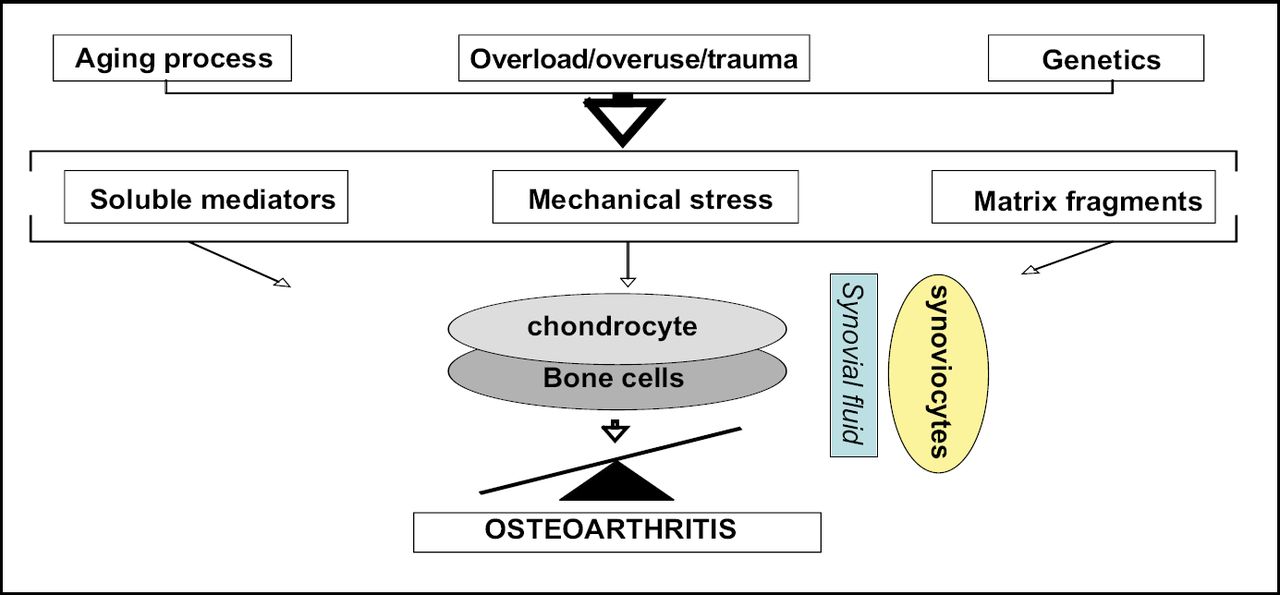
Until the late 1980's osteoarthritis (OA) was thought of as a passive consequence of “wear and tear”, but thanks to recent advances we now know that it is a cell driven mechanism based on a variety of factors (Figure 1). It is not a degenerative disease that primarily affects cartilage, as previously thought, but a pro-inflammatory disease that affects multiple tissues. According to Francis Berenbaum, MD, Hospital Saint-Antoine, Paris, “In the past we viewed osteoarthritis as an inevitable fate—but in fact it's not—it is a biological challenge open to therapeutic intervention”.
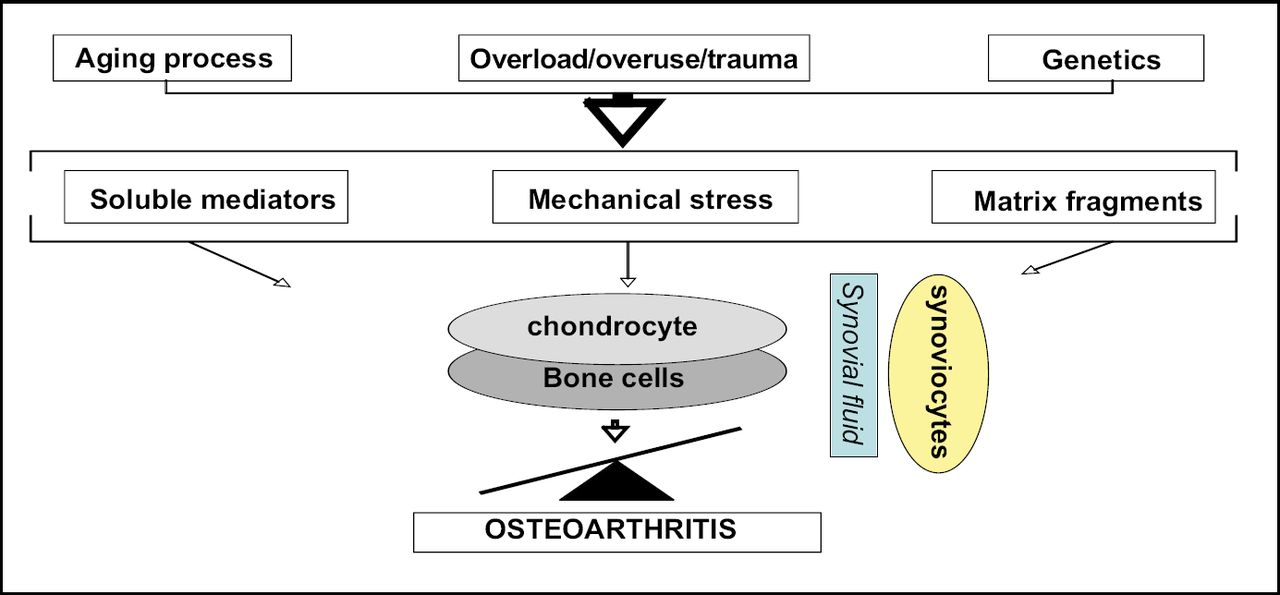
Osteoporosis. Cell Driven Mechanism.
Maxime Dougados, MD, Hopital Cochin, Paris, presented an overview of some of the work that has been done to identify prognostic indicators for progression of hip and knee arthritis and about the markers of disease.
Early research showed that changes in joint space width of at least 0.6 mm could be used to define radiologic progression of hip OA. Clinical parameters such as pain, functional impairment and treatment level (eg, NSAID and analgesic intake) were also significantly (p<0.0001) associated with disease progression [Dougados M et al. Ann Rehum Dis 1996; Gossec L et al. Ann Rheum Dis 2005; Lane et al. Arthritis Rheum 2004].
Ayral et al [Osteoarthritis Cartilage 2005] have shown that in knee OA, synovitis may be a predictor of increased degradation of medial chondropathy and Belo et al [Arthritis Rheum 2007] found that generalized OA and the level of hyaluronic acid appeared to be associated with radiologic progression.
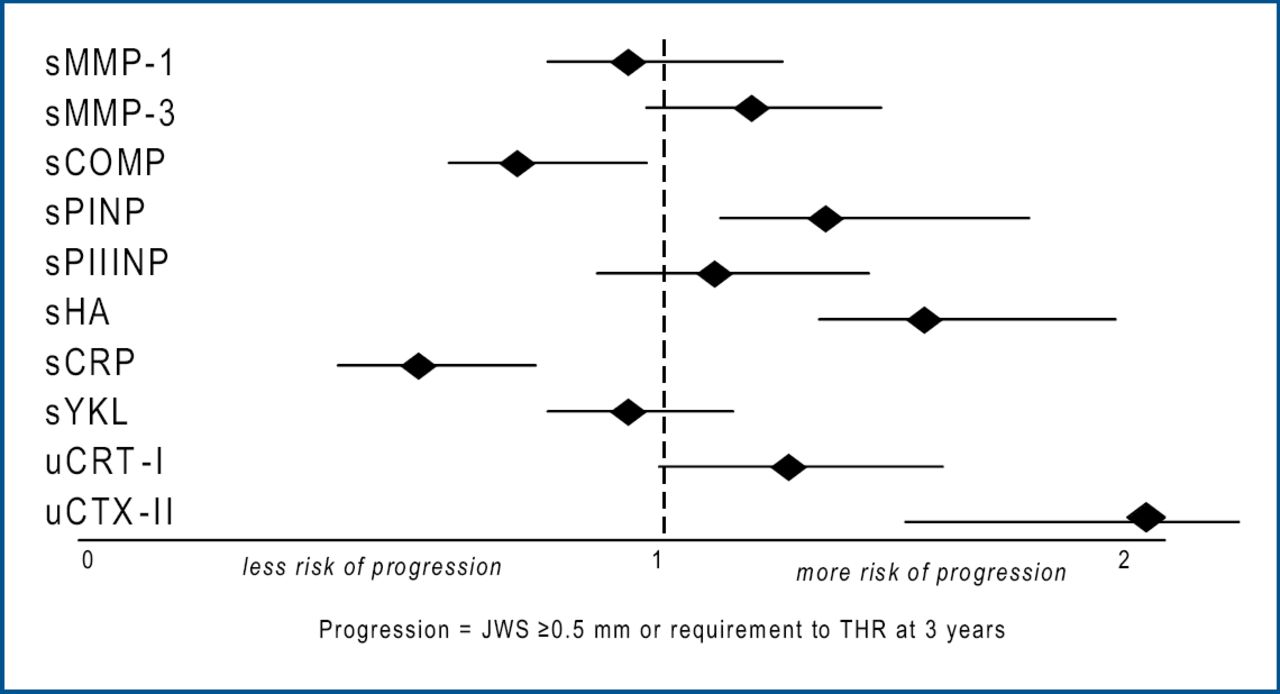
Recently, investigators have begun to explore the potential of biological markers as predictors of progression. Results of a study conducted by Mazières et al [Ann Rheum Dis 2006] to assess the potential value of systemic markers of bone, cartilage, and synovium indicated that combined measurements of uCTXII and sHA may have utility in the prediction of structural progression of hip OA (Figure 2). In another study, treatment with risedronate reduced the levels of two markers of cartilage degradation (NTX-1 and CTX-1), despite failing to meet the primary endpoint of the study, ie, reducing the signs/symptoms and slowing disease progression. These findings might indicate that the markers do not correlate with the disease symptoms, or that the study structure or design was not optimal.
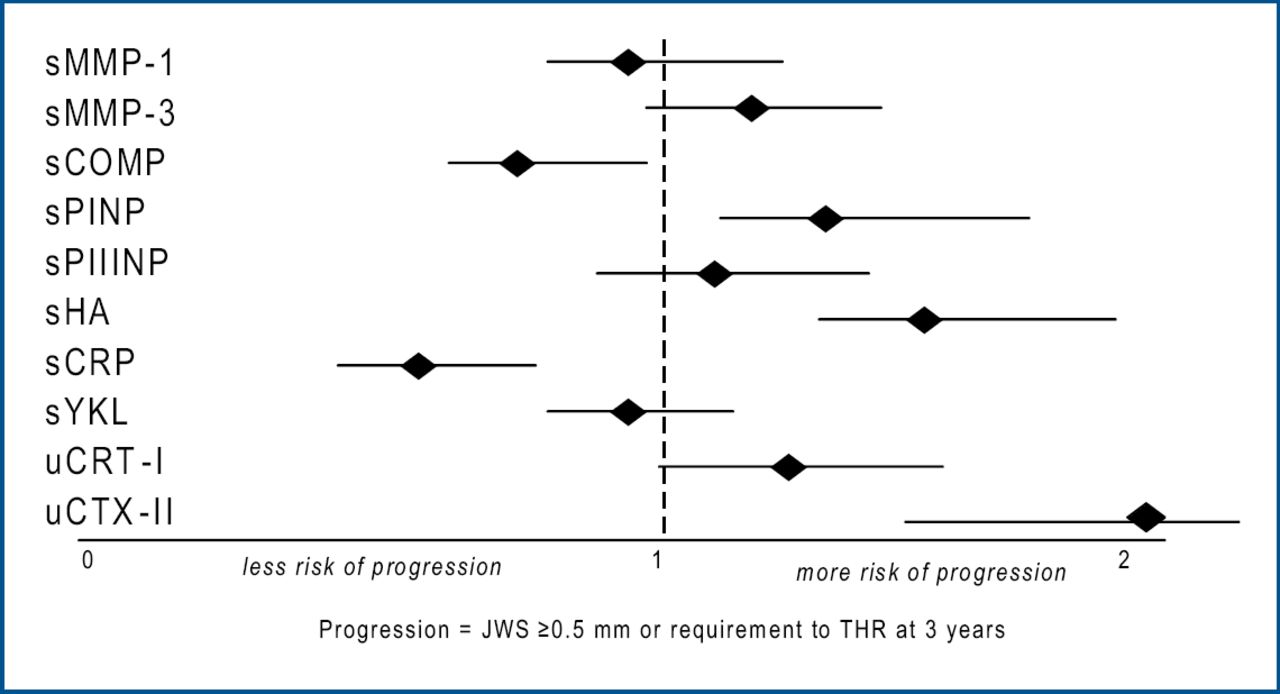
Value of Prognostic Markers in OA.
According to Prof. Dougados, “The markers of osteoarthritis progression can be split into two categories: those that are modifiable (eg, inflammation and obesity) and those that are not (eg, age, structure). A better understanding of the mechanisms of these markers might be important before targeting therapies, as well as in the early stages of the development of new treatments.”
Hand OA most commonly affects small finger joints and the joint at the base of the thumb. Treatment options include oral medication, injections, splinting, and surgery. Despite the frequency of its diagnosis, knowledge about its progression and effective therapies is lacking.
Stella Botha-Scheepers, MD, Leiden University, The Netherlands, presented the results of the GARP (Genetics, ARthrosis and Progression) trial, a 2-year follow-up study conducted to assess the responsiveness of currently available outcome measures in a series of patients with hand OA.
Study participants were middle-aged (mean age 60.5 years). Most were women (78.5%). Pain intensity upon lateral pressure in the DIP, IP, PIP and CMC 1 joints was graded on a four-point scale. Self-reported hand pain and functional limitations were assessed with the pain and function subscales of the Australian/Canadian Osteoarthritis Hand Index (AUSCAN LK 3.0). Standardized radiographs of the hands were obtained at baseline and after 2 years. Right and left DIP joints, IP joints of the thumbs, PIP joints and CMC 1 joints were scored (0–3) for osteophytes and joint space narrowing (JSN).
A total of 172 patients (91%) completed the 2-year follow-up, at which time significant increases in pain intensity on lateral pressure standard response mean (SRM; 0.67), AUSCAN pain scores (SRM 0.25) and AUSCAN function scores (SRM 0.23) occurred. Statistically significant radiological progression was detected in 20% of patients, in terms of joint space narrowing (SRM 0.34) and osteophytes (SRM 0.35).
Dr. Botha-Scheepers commented: “The findings of this study underline the critical need for early, effective intervention in hand OA to prevent irreversible progression….”
In knee OA, there are several radiographic views and scoring methods available to identify structural damage. According to results of a study presented by Laure Gossec, MD, Cochin Hospital, Paris V University, measuring joint space width in millimeters on x-rays of the semi-flexed knee is the most accurate way of evaluating structural damage in patients with knee OA.
The objective of this study was to compare psychometric properties of three scoring methods in knee OA and to compare extended versus semi-flexed views.
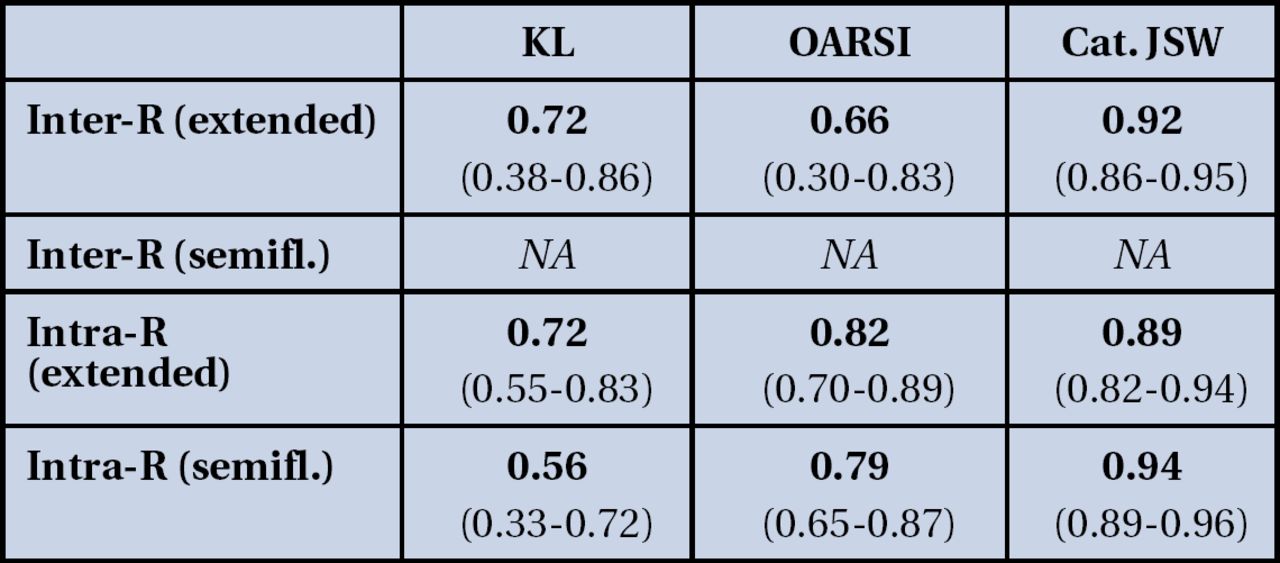
Data for 1,759 radiographs of fully extended or semi-flexed knees were gathered from five databases and analyzed using semi-quantitative scores: the Kellgren and Lawrence (KL) scale, and the Osteoarthritis Research Society International (OARSI) joint space width (JSW) scale. They were also assessed using precise measurement of JSW in millimeters, which was then analysed as a semi-quantitative scale.
The highest inter-rater reliability was found in the precise measurement of JSW in extended knees, Intraclass Correlation Coefficient (ICC) 0.92 (0.86–0.95) vs 0.72 (0.38–0.86) in the KL scale, and 0.66 (0.30–0.83) using the OARSI scale. Intra-rater reliability was also high for categorical JSW in extended and semi-flexed views, indicating that these measures are highly reproducible across readings and across readers (Figure 3). Sensitivity to change was highest for categorical JSW in the semi-flexed knee (SRM 0.49 vs SRM 0.22 for the KL scale, and 0.34 for the OARSI scale), indicating that JSW on semi-flexed views is a better detector of change over time or after treatment than the other techniques.
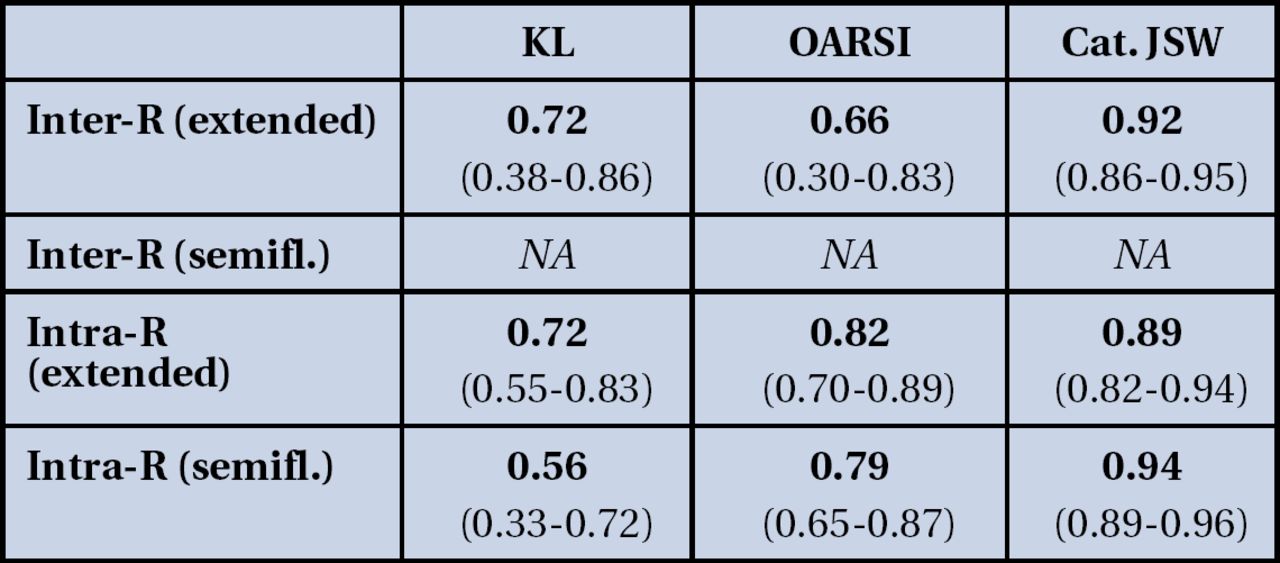
Reliability: Intraclass Correlation Coefficients.
Dr. Gossec commented, “Measuring joint space width, in particular in the semi-flexed knee, has been shown to be the most reliable and responsive way to determine structural damage severity in knee OA trials, since overall, reliability and responsiveness were higher for JSW (in particular on semi-flexed view) than for the other scoring techniques.”
Prof. Wim B. van den Berg, MD, University Hospital Nijmegen, The Netherlands, provided a glimpse into the future of OA treatment via animal model studies that are exploring novel therapeutic targets in OA. Among these are IL-1 and the role of activated macrophages and degradative enzymes such as ADAMS5 and stromelysin. Novel receptors currently being investigated include the toll like receptors (TLRs) and the receptors of advanced glycation end products. TLRs are expressed on chondrocytes and synoviocytes. When activated, they drive the degradative enzymes. Advanced glycation end products are the result of non-enzymatic glycation of proteins, such as collagen. They accumulate with age and result in pathologic stiffening of cartilage and extracellular matrix.
These ongoing investigative efforts hold promise for the development of novel drugs both for the management of pain as well as retarding the OA process.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.