

Summary
Clinical practice guidelines are intended to establish greater consistency of treatment and improve quality of care. To be most useful, guidelines should be updated regularly to include important data from clinical trials. Each year at its annual meeting, the European Society of Cardiology releases several new or updated guidelines. This year, one new set of guidelines was issued and three others were updated.
- Cardiology Guidelines
- Coronary Artery Disease
- Lipid Disorders
- Hypertensive Disease
Clinical practice guidelines are intended to establish greater consistency of treatment and improve quality of care. To be most useful, guidelines should be updated regularly to include important data from clinical trials. Each year at its annual meeting, the European Society of Cardiology (ESC) releases several new or updated guidelines. This year, one new set of guidelines was issued and three others were updated.
Peripheral Artery Disease (PAD)
A substantial number of patients with coronary artery disease (CAD) also have cerebrovascular and/or lower extremity artery disease [Steg PG et al. JAMA 2007]. To aid in assessing patients with CAD for atherosclerosis at other sites, the ESC has issued its first set of guidelines for the diagnosis and treatment of PAD [Tendera M et al. Eur Heart J 2011]. The guideline overview was presented by Michal Tendera, MD, PhD, Medical University of Silesia, Katowice, Poland, and Victor Aboyans, MD, PhD, Dupuytren University Hospital, Limoges, France.
According to the new guidelines, a general diagnostic approach should include a complete medical history that focuses on a review of vascular beds and their specific symptoms, a systematic physical examination, and laboratory assessments to detect major risk factors of cardiovascular disease (CVD). The ankle-brachial index and duplex ultrasound are extremely useful diagnostic tools. Other noninvasive diagnostic modalities include computed tomography (CT) angiography and magnetic resonance angiography. Angiography, although considered the diagnostic gold standard in the past, is now used almost exclusively during endovascular procedures. The new guidelines stress that in all patients with PAD, secondary prevention should be implemented (Table 1). The major portion of the new guidelines is the site-specific section, which covers extracranial carotid and vertebral artery disease, upper extremity artery disease, mesenteric artery disease, renal artery disease, lower extremity artery disease, and multisite artery disease. For each condition, there is a detailed discussion of diagnosis and treatment modalities (medical therapy, surgery, and endovascular techniques). Differences in approaches for symptomatic and asymptomatic patients are also presented. The guidelines also provide direction for the management of patients with multisite artery disease.
General Treatment Rules in Patients with PAD.
Acute Coronary Syndromes Without ST Elevation
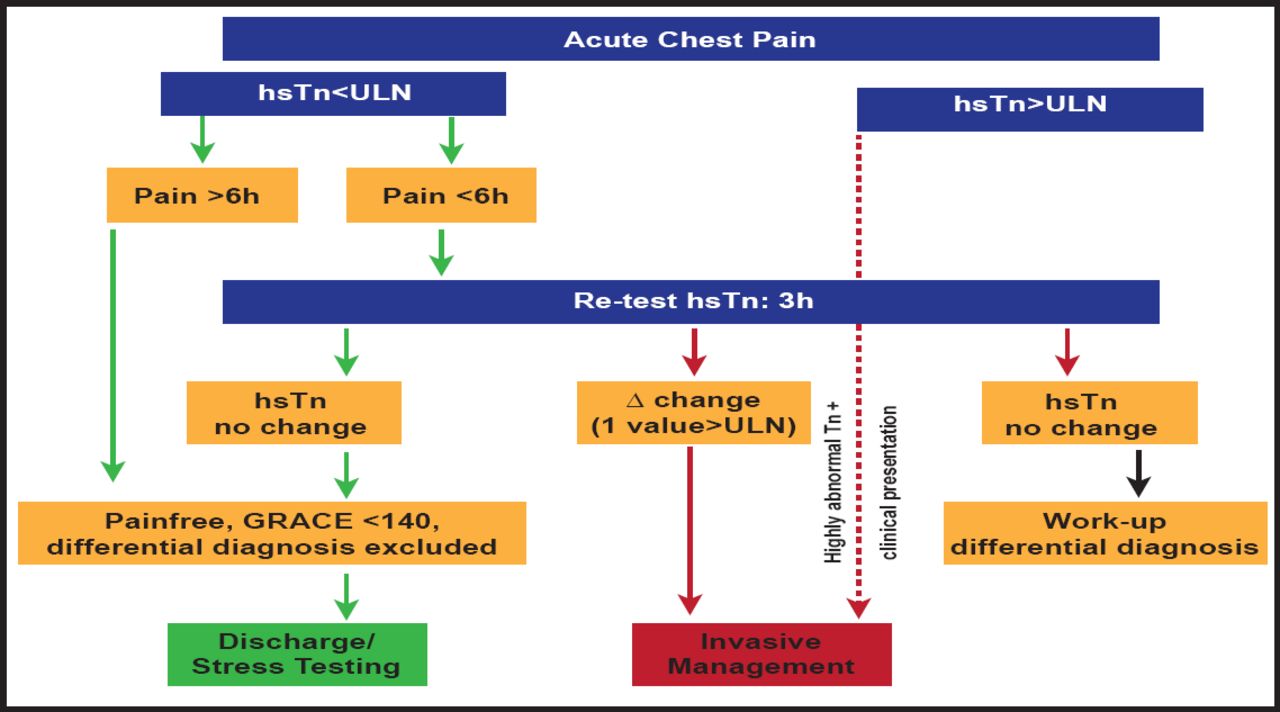
The 2011 ESC Guidelines for the management of acute coronary syndromes (ACS) in patients who present without persistent ST-segment elevation [Hamm W et al. Eur Heart J 2011] were presented by Christian W. Hamm, MD, Kerckhoff Heart Center, Bad Nauheim, Germany. Important changes to the 2007 version of these guidelines involve diagnosis, risk stratification, medical treatment, and revascularization (Table 2). For the first time, it is recommended that patients with ACS be admitted, preferably to a dedicated chest pain or coronary care unit. The CRUSADE score is now recommended in addition to the GRACE score for prognostic assessment. The revised guidelines recommend that all patients receive an echocardiogram and that in certain patients, coronary CT angiography should be considered as an alternative to angiography to exclude ACS. Highly sensitive troponin (hsTn) tests are now included in the guidelines, and a new rapid rule-out protocol has been established for when these tests should be used (Figure 1). Under medical treatments, a proton pump inhibitor, in combination with dual antiplatelet therapy, is now recommended in selected patients, and both prasugrel and ticagrelor have been added to the treatment algorithm. Anticoagulation is recommended for all ACS patients in addition to antiplatelet therapy. The anticoagulation should be selected, based on both ischemic and bleeding risk and according to the efficacy-safety profile of the selected agent. Fondaparinux remains the preferred anticoagulant due to its favorable efficacy-safety profile. Enoxaparin is recommended when fondaparinux is not available. Bivalirudin plus provisional GP IIb/IIIa receptor inhibitors is recommended as an alternative to unfractionated heparin plus GP IIb/IIIa receptor inhibitors in patients with an intended urgent or early invasive strategy, particularly those who are at high risk of bleeding. The decision-making algorithm for invasive treatment has been modified from the 2007 guidelines to include the provision for an early invasive strategy in selected patients.
What's New in the 2011 Guidelines?

Rapid Rule-Out of ACS with hsTn.
hsTn=highly sensitive troponin; ULN=upper limit of normal. Reproduced with permission from the European Society of Cardiology.
Cardiovascular Disease During Pregnancy
Between 0.2% and 4% of all pregnancies in industrialized nations are complicated by CVD. This number is rising due to older age in pregnancy and successful surgery for congenital HD. Hypertension (6% to 8% of pregnancies; serious complications infrequent), congenital HD (the cause of 75% to 82% of cardiac complications in the western world and only 9% to 19% outside Europe and North America), valvular HD (present in only 15% in industrialized countries but dominant in developing countries; mitral stenosis is most frequent), coronary HD (rare but increasing), myocardial disease, and cardiomyopathy (rare but can cause severe complications; strong variation by country) are some of the CVDs that are seen during pregnancy. Vera Regitz-Zagrosek, MD, Deutsches Herzzentrum Berlin, Berlin, Germany, provided an overview of the ESC Guidelines on the management of CVD during pregnancy, which for the first time includes graded recommendations [Regitz-Zagrosek V et al. Eur Heart J 2011]. There are new recommendations in the guidelines concerning genetic testing, which should be performed if cardiomyopathy or channelopathies are suspected, if other family members are affected, or in the presence of dysmorphic features or other congenital abnormalities. The guidelines cover maternal diagnosis (including tests that can be modified by pregnancy and radiation doses for procedures that are needed for diagnosis), fetal assessment (by ECHO and biophysical profile), maternal interventions (percutaneous coronary intervention and cardiac surgery), infective endocarditis, contraception, termination of pregnancy, and in vitro fertilization. There are extensive recommendations on the timing and mode of delivery, general recommendations on risk estimation and high-risk states, and contraindications for pregnancy. Essential messages are summarized in Table 3.
General Recommendations/Essential Messages.
Dyslipidemia
Željko Reiner, MD, University of Zagreb, Zagreb, Croatia, and Alberico L. Catapano, PhD, MD, University of Milan, Italy, presented the 2011 ESC/EAS guidelines for the management of dyslipidemia. Changes in plasma lipoprotein levels, whether alone or in combination with other CV risk factors, may affect the development of atherosclerosis; thus, optimal management of dyslipidemia is an essential and integral part of CVD prevention. In these guidelines, the prevention and treatment of dyslipidemia are considered within the broader framework of CVD prevention. There is less emphasis on target total cholesterol and more emphasis on low-density lipoprotein (LDL) levels, with a new lower target for LDL of <1.8 mmol/L (<70 mg/dL) that is recommended for patients who have the highest risk. High-density lipoprotein (HDL) is introduced as an important risk factor. Risk is assessed as being relative versus the more commonly used dichotomized approach (Table 4); thus, the level and timing of intervention and the targets (Table 5) are related to a particular combination of CV risk score and LDL level. Lifestyle changes, a major component of the approach at all levels, are also outlined, as are strategies to assist in medication compliance. The guidelines also provide specific recommendations for selected patient populations, including women, the elderly, and individuals with diabetes.
LDL Target Recommendations.
Intervention Strategies as a Function of Total CV Risk and LDL-C Level.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.