

Summary
This article reviews the highlights of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults.
- lipid disorders
- prevention & screening
- cardiology guidelines
- coronary artery disease
Roger S. Blumenthal, MD, Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore, Maryland, USA, reviewed the highlights of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults [Stone NJ et al. Circulation. 2013].
AN OVERVIEW OF THE 2013 ACC/AHA GUIDELINES
The guidelines now assess stroke in addition to myocardial infarction (MI) and include separate equations for nonwhite populations. The guidelines also identify 4 statin benefit groups, including a large eligibility group (threshold risk ≥ 7.5%) that could be treated with statins after a risk discussion. There are no low-density-lipoprotein cholesterol (LDL-C) or non-high-density-lipoprotein cholesterol (HDL-C) treatment targets due to the lack of definitive clinical trial evidence. The 2013 prevention guidelines include an easy-to-use atherosclerotic cardiovascular disease (ASCVD) Risk Estimator.
The guideline panel identified that patients with a risk ≥ 7.5% might benefit from a statin; however, they cautioned that the net benefit from a treat-to-target strategy for cholesterol remains unknown and that such an approach may result in suboptimal statin therapy or an increased adverse event risk.
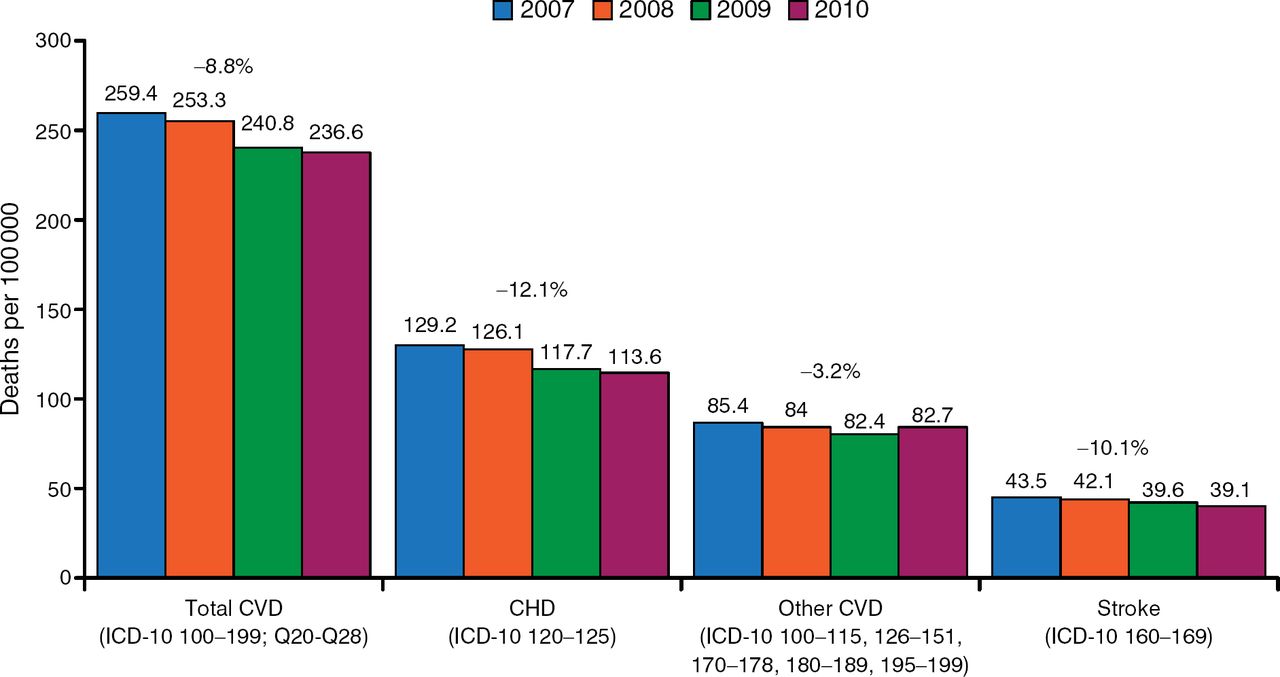
Recent data suggest that the increase in statin use in the United States is likely associated with the declining death rate for all types of cardiovascular (CV) events (Figure 1).

US Death Rate for Cardiovascular Disease Decreasing
CHD, congestive heart disease; CVD, cardiovascular disease; ICD, International Classification of Diseases.
Source: CDC National Vital Statistics Report.
This decline may account for some of the overestimation of CVD risk, which can be as high as 75% to 150% with some risk assessment tools [Ridker PM, Cook NR. Lancet. 2013]. Even the validation cohorts used in the new guidelines showed that the new risk estimator overestimated actual risk. Observed and predicted 5-year ASCVD risks were similar in another study, in which pooled cohort risk equations were developed to assess ASCVD, indicating good calibration and moderate discrimination in the population for which they were designed to be used [Muntner P et al. JAMA. 2014]. Some of the variance might be explained by changing patterns of risk within more contemporary populations and differences in socioeconomic status [Cook NR, Ridker PM. JAMA Intern Med. 2014].
The 2013 guidelines match statin assignment to total plaque burden better than the older guidelines and substantially increase the number of adults who are eligible for preventive statin therapy [Johnson KM et al. J Am Coll Cardiol. 2014]. The increase is seen mostly among older adults without CVD [Pencina MJ et al. N Engl J Med. 2014]; however, approximately 11% more individuals aged ≥ 40 years are now eligible for statin therapy.
Clinical guidelines are still evolving, and in the future, they may include a coronary calcium score as a risk factor combined with non-HDL. When using the guidelines, Dr Blumenthal advised that clinicians should consider patient preference, the precision of the patient's risk estimate, how motivated the patient is to participate in his or her treatment program, potency of treatment, and price. Finally, for high-risk patients and those with a lower than anticipated LDL-C response to statins, nonstatins can be used, but preference is given to those clearly at high risk.
ADDITIONAL AHA/ACC GUIDELINES TO REDUCE CVD RISK ISSUED IN 2013
In addition to the blood cholesterol guidelines [Stone NJ et al. Circulation. 2013], guidelines for lifestyle management [Eckel RH et al. Circulation. 2013] and overweight and obesity in adults [Jensen MD et al. Circulation. 2013] to reduce CVD risk were also issued by AHA/ACC in 2013. Lawrence J. Appel, MD, MPH, Johns Hopkins University, Baltimore, Maryland, USA, reviewed some of the data that formed the basis for these recommendations.
For CVD prevention, the lifestyle guidance stresses adoption of a Mediterranean or Dietary Approaches to Stop Hypertension (DASH)-style diet, weekly aerobic physical activity of moderate to vigorous intensity, and smoking cessation. The diet recommendations were based on the PREDIMED trial [Estruch R et al. N Engl J Med. 2013], which showed that a Mediterranean diet supplemented with extra-virgin olive oil or nuts reduces the incidence of major CV events.
Sodium guidelines remain in place based on the robust body of evidence linking sodium with elevated blood pressure (BP)—as sodium intake rises, so does blood pressure in a progressive dose-response fashion. The best available evidence also supports a direct relationship of sodium intake with CVD events. In the Trials of Hypertension Prevention, there was a direct relationship between urine sodium excretion (based on the average of multiple 24-hour urine collections) and CVD events [Cook MR et al. Circulation. 2014].
In another study, an intensive lifestyle intervention focusing on weight loss surprisingly did not reduce the rate of CV events in overweight or obese adults with type 2 diabetes (P = .51) [Look AHEAD Research Group. N Engl J Med. 2013]. However, Dr Appel pointed out that participants in the study received medical care for their risk factors, leading to a convergence of weight and CVD risk factors in the randomized groups.
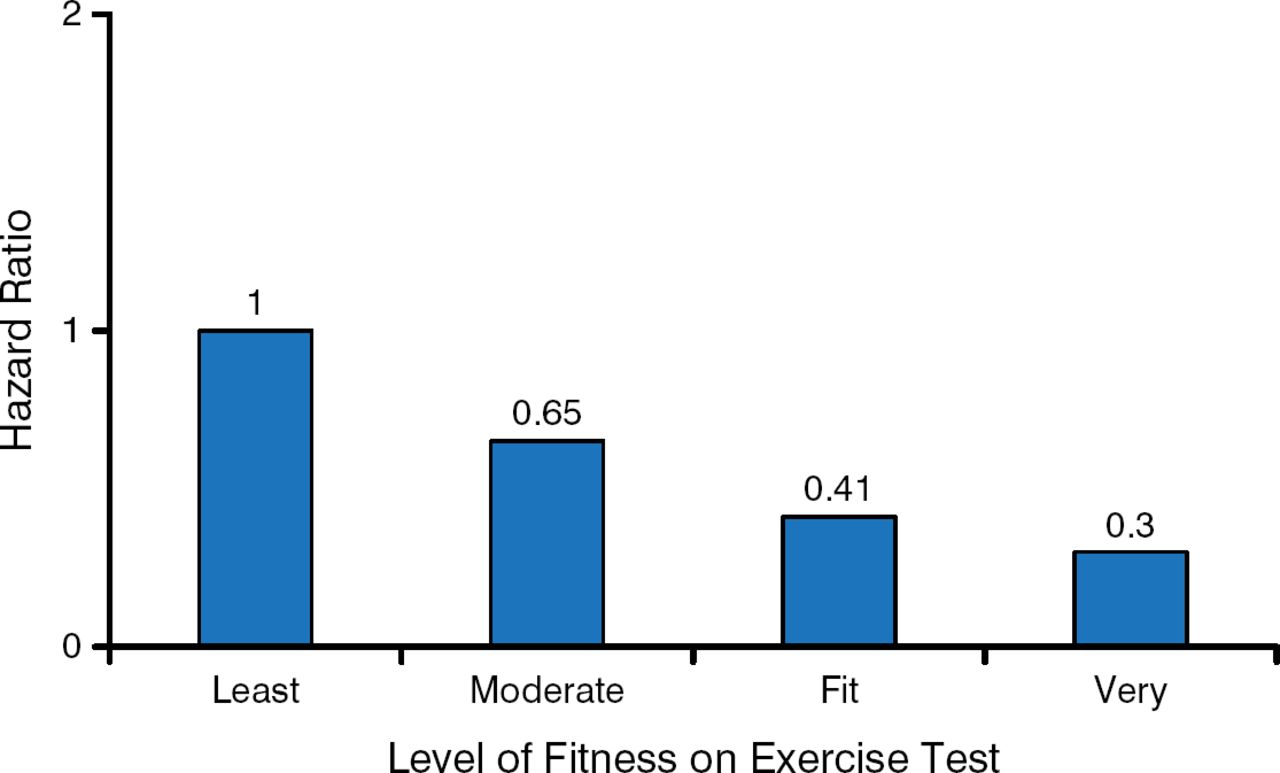
As for the role of exercise, in an intriguing study of dyslipidemic individuals, better fitness was associated with a reduced risk of death, both in statin users and in those who were not taking a statin (Figure 2) [Kokkinos PF et al. Lancet. 2013].

Greater Fitness in Statin Users Lowers Death Risk
Source: Kokkinos PF et al. Lancet. 2013.
Reproduced with permission from LJ Appel, MD, MPH.
More research is needed regarding the benefits of behavioral therapy delivered by primary care physicians. However, in a study conducted by Dr Appel and colleagues [N Engl J Med. 2011], they found that obese patients achieved and sustained clinically significant (∼ 4 kg, P < .001) weight loss during a period of 24 months if those patients received either an in-person support or a remotely delivered weight loss intervention. He concluded that lifestyle modification is an important component of prevention and control of CVD, and that physicians should promote lifestyle change in their patients.
IMPORTANCE OF ASCVD PREVALENCE IN APPLYING CLINICAL RISK SCORES
Samia Mora, MD, MHS, Brigham and Women's Hospital, Boston, Massachusetts, USA, reviewed 3 topics that affect the generalizability of the 2013 ACC/AHA risk score.
When making clinical decisions, clinicians often judge the probability of disease, but this judgment may be inaccurate due to differences in disease prevalence in different populations, and lack of discriminating cases from controls in the new setting. Adjusting the prediction score to the local prevalence and the pretest probability of disease will make the prediction more accurate.
The Women's Health Initiative (WHI) included 3 controlled trials (hormone therapy, calcium and vitamin D, and dietary modification) and 1 observational study. Dr Mora is currently conducting an assessment of statin use in the WHI by risk category. The results are expected to be published next year.
There is a residual vascular risk during statin therapy. During a 5-year follow-up, 1 of 5 patients with prior ASCVD who are taking statins will have a recurrent event; 1 in 10 patients without prior ASCVD will have a first event [Baigent C et al. Lancet. 2005]. In a meta-analysis of 8 statin trials, LDL-C, non-HDL-C, and apolipoprotein B were each significantly (P < .001) associated with risk of future major CV events [Boekholdt SM et al. JAMA. 2012]. According to Dr Mora, the ability to detect the higher-risk individuals who will have an ASCVD event during statin therapy can be improved by attending to these biomarkers, and the lower the atherogenic particles, the better.
David A. Wood, MD, Imperial College of London, London, United Kingdom, provided a European perspective on the 2013 ACC/AHA Cholesterol Guideline [Stone NJ et al. Circulation. 2013].
Dr Wood believes that the statin intervention criteria (> 7.5% throughout 10 years vs about 20% in the European guidelines [Perk J et al. Eur Heart J. 2012]) is set too low. He noted that the European approach is to focus on total CV risk assessment and risk management, consisting of lifestyle intervention (smoking cessation, diet, weight management, and physical activity), controlling clinical risk factors (BP, lipid, and glucose), and assuring adherence to cardioprotective drug therapies. In contrast, the ACC/AHA guideline's use of assessing and treating individual risk factors such as hypertension, hyperlipidemia, and hyperglycemia creates a silo approach to a multifactorial risk problem. Since the publication of the ACC/AHA guideline, there have been 2 reports that suggest it offers a silo approach to lipid therapy [Jacobson TA et al. J Clin Lipidol. 2014; James PA et al. JAMA. 2014].
Dr Wood added that the guideline recommendations for high-intensity (> 50% LDL-C-lowering) and moderate-intensity (30% to 50%) statin therapy for secondary and primary prevention of ASCVD are not appropriate for all patients or for lipid management.
Dr Wood says he sees no proof that the ACC/AHA guideline is cost-effective, because it does not consider the cost associated with screening adult populations to estimate total CVD risk. He also believes that they fail to embrace the potential value of lifetime risk, whereas the European guidelines encourage behavioral changes toward a healthier lifestyle.
Dr Wood concluded that there is a need for integrated guidelines for secondary and primary prevention of CVD that involve the major stakeholders to agree to a common agenda that will benefit all patients.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.