

Summary
A small randomized study failed to demonstrate the superiority of renal sympathetic denervation (RSD) compared with medical therapy in achieving lowered blood pressure (BP). However, while systolic BP was decreased 6 months post denervation in all patients, the decrease was significant only for the per-protocol cohort.
- Hypertensive Disease
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Hypertensive Disease
- Cardiology
- Interventional Techniques & Devices
- Cardiology Clinical Trials
A small randomized study failed to demonstrate the superiority of renal sympathetic denervation (RSD) compared with medical therapy in achieving lowered blood pressure (BP). However, while systolic BP was decreased 6 months post denervation in all patients, the decrease was significant only for the per-protocol cohort. The findings, which are provocative rather than definitive, were reported by Steffen Desch, MD, University of Lübeck, Lübeck, Germany.
While percutaneous RSD might be effective in lowering BP in patients with severe resistant hypertension, the applicability when BP is only slightly elevated is unclear. This study was designed to assess the issue. Seventy-one patients with resistant, yet only mildly elevated BP were randomized to RSD or a sham procedure. RSD used the Symplicity Flex Catheter for 4 to six 2-minute circumferential ablations in a distal-to-proximal direction for each renal artery. The procedures were done by experienced personnel who had performed at least 20 procedures prior to the study. The sham procedures consisted of an angiography of renal arteries as well as an invasive simulation of RSD. The surroundings and equipment were the same as for the genuine procedure. Intravenous saline was used instead of pain medication.
The inclusion criteria were a mean daytime systolic BP of 135 to 149 mm Hg determined from a 24-hour ambulatory BP measurement (ABPM) and/or mean daytime diastolic BP of 90 to 94 mm Hg, use of a stable anti-hypertensive regimen that had not been changed for the 4 weeks preceding study randomization that consisted of ≥ 3 drugs including an optimal dose of a diuretic, and age ≥ 18 to ≤ 75 years. Exclusion criteria were ABPMs less than or more than the prespecified mean systolic and diastolic BPs, anatomic restriction for RSD, glomerular filtration rate < 45 mL/min/1.73 m2, any change in BP medication in the 4 weeks prior to randomization, and subject resistance to maintenance of the medication regimen. The primary end point was the change in 24-hour systolic BP at 6 months in the intention-to-treat (ITT) cohort.
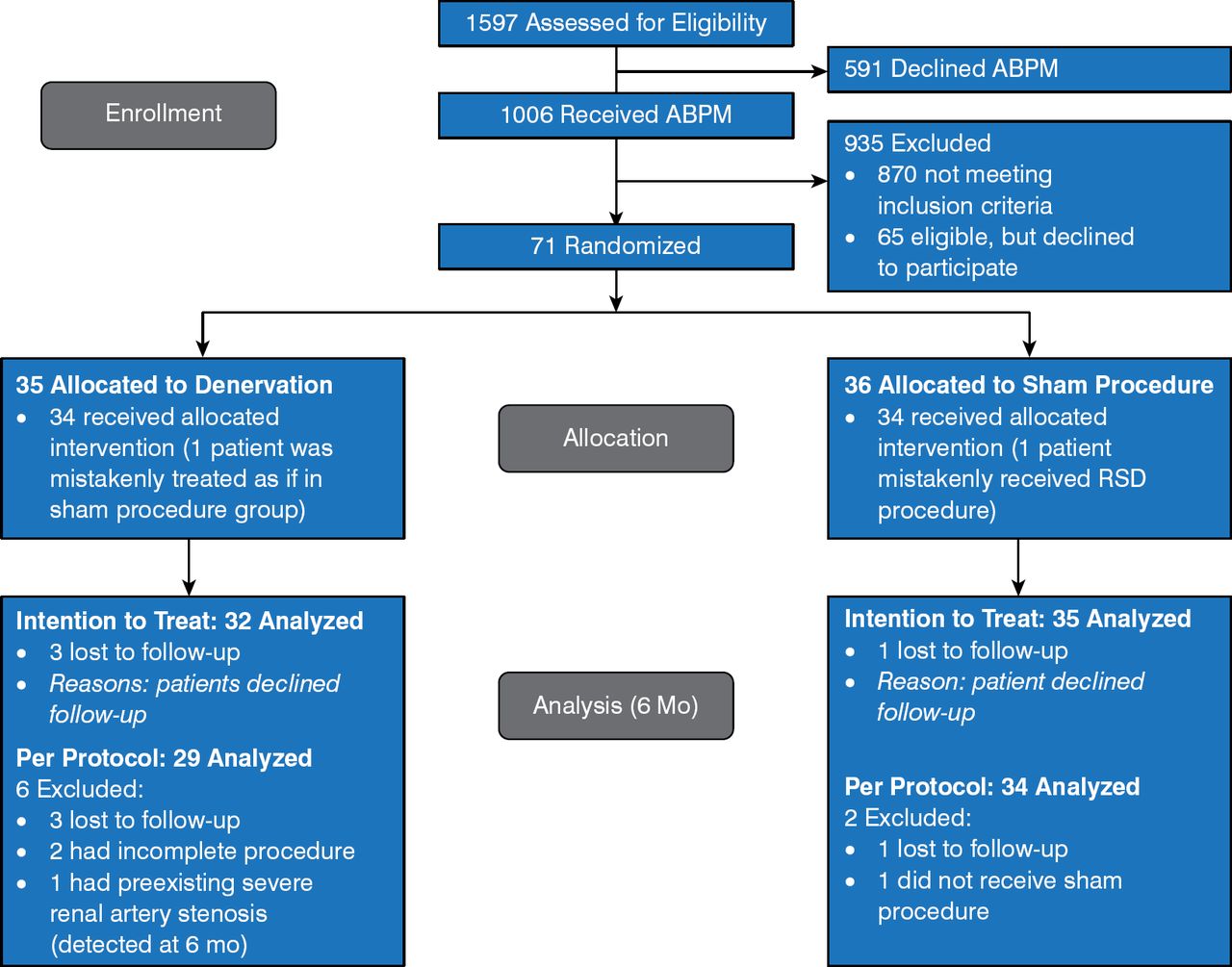
Of the 1597 patients who were assessed, 71 were randomized to RSD (n = 35) or sham procedure (n = 36). At the 6-month analysis, the ITT population comprised 32 in the RSD group and 35 in the sham group; 29 and 34 patients in the per-protocol cohort, respectively (Figure 1).

Flow Chart of the Study
ABPM, ambulatory blood pressure measurement; RSD, renal sympathetic denervation.
Reproduced with permission from S Desch, MD.
The 2 groups were similar at baseline in demographic and clinical parameters, with the exception of age (64.5 ± 7.6 years in the RSD group, 57.4 ± 8.6 years in the sham group; P < .001). The groups were also comparable in baseline medications (diuretic, β-blocker, calcium channel blocker, and angiotensin-converting enzyme receptor blocker in order of prevalence).
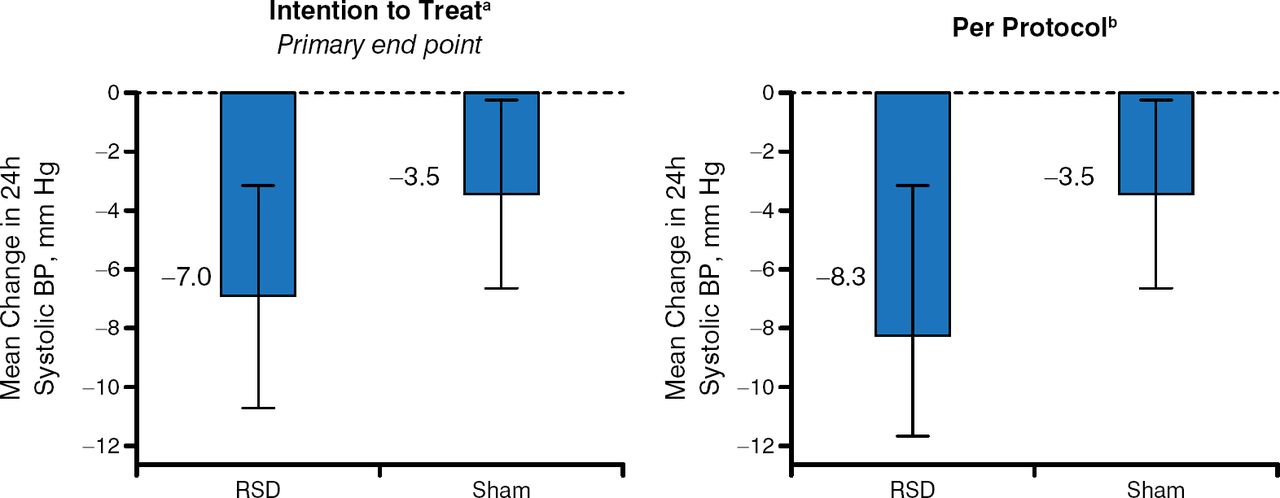
The primary end point was not met, with no significant difference in mean change of 24-hour systolic BP from baseline to 6 months in the ITT population (P = .15). The difference was significant in the per-protocol population, favoring RSD (P = .042; Figure 2).

Primary End Point Results
BP, blood pressure; RSD, renal sympathetic denervation.
a P = .15 for between-group comparison; b P = .042 for between-group comparison; Error bars show 95% CI.
Reproduced with permission from S Desch, MD.
Study limitations included small sample size, lack of assessment of medication adherence in the absence of urine analysis, and lack of an objective assessment of the success of blinding. Also, the finding of significance only in per-protocol patients necessitates further study to draw a definitive conclusion concerning the efficacy of RSD.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.