

Summary
Weight loss can reduce the effects of risk factors for atrial fibrillation (AF) and AF symptoms. Thus, weight reduction should be an important facet in the management of the obese patient with AF.
- Arrhythmias
- Obesity
- Prevention & Screening
- Cardiology & Cardiovascular Medicine
Weight loss can reduce the effects of risk factors for atrial fibrillation (AF) and AF symptoms according to Prashanthan Sanders, MBBS, PhD, University of Adelaide and the Royal Adelaide Hospital, Adelaide, Australia. Thus, weight reduction should be an important facet in the management of the obese patient with AF.
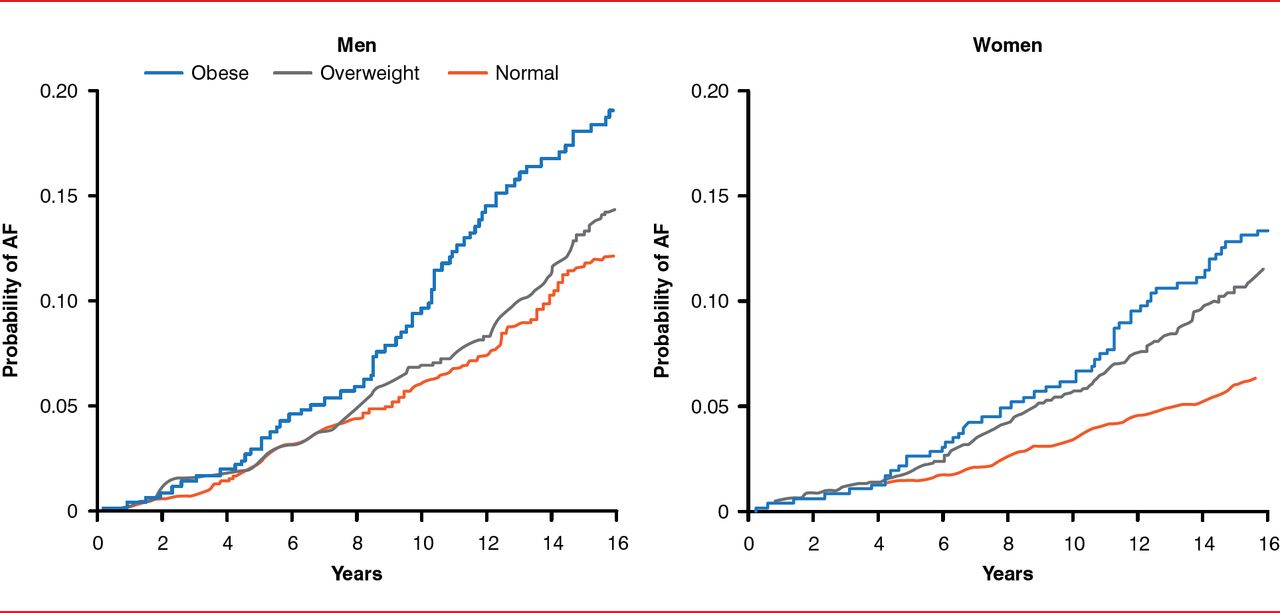
The severity of sleep apnea is partially related to body mass index (BMI), and obesity is associated with the severity of sleep apnea [Gami AS et al. J Am Coll Cardiol 2007]. Obesity has also been clinically linked in humans with a decreased refractory period (especially in the pulmonary vein), decreased left atrial strain, increased left atrial pressure, and volume [Munger TM et al. J Am Coll Cardiol 2012]. In sheep, obesity has been associated with progressively increasing atrial fibrosis and electrical changes in the myocardium [Abed HS et al. Heart Rhythm 2013]. Women who are obese (BMI >30 kg/m2) are at greater risk of AF, compared with individuals with BMI <30 kg/m2 who maintain or reduce their weight [Tedrow UB et al. J Am Coll Cardiol 2010]. For both genders, the probability of AF increases with time, especially in obese men (Figure 1) [Wang TJ et al. JAMA 2004].

Relationship of Obesity and Atrial Fibrillation
Reproduced from Wang TJ et al. Obesity and the risk of new-onset atrial fibrillation. JAMA 2004;292(20):2471–2477. © 2004 American Medical Association. All rights reserved.
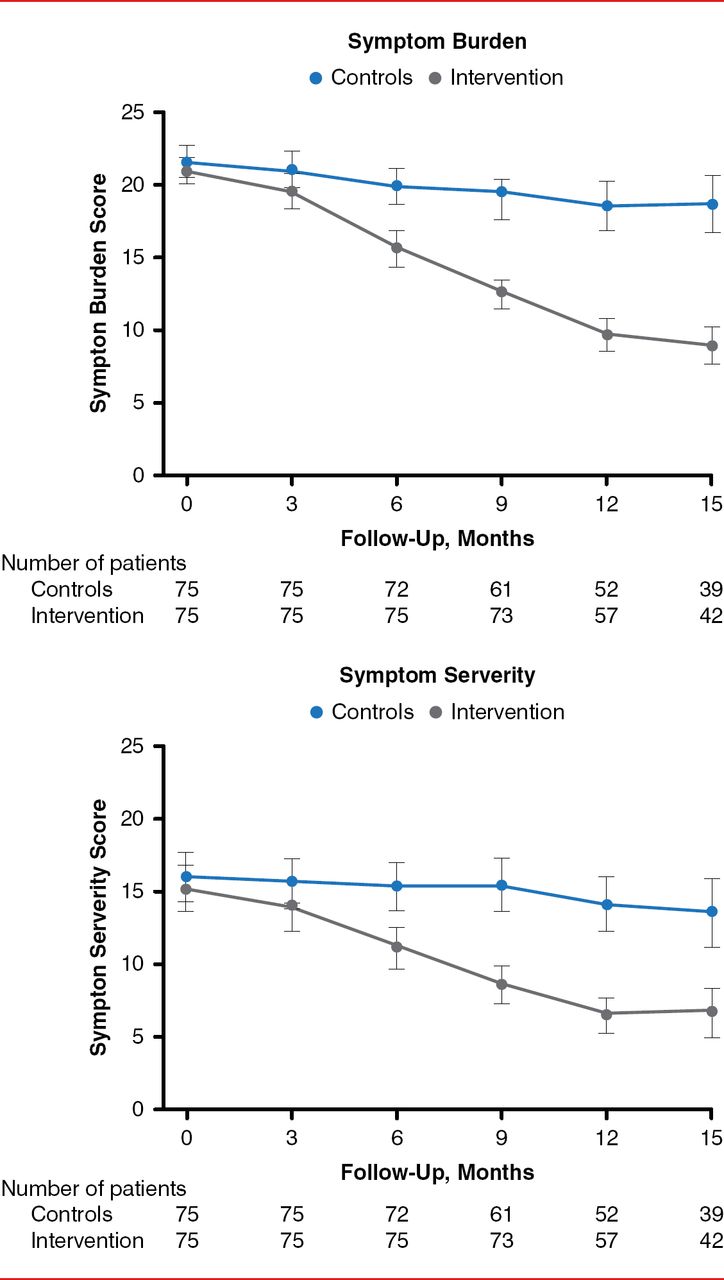
Animal studies have suggested that obesity significantly increases vulnerability to AF and that this risk can be reduced with weight loss. These data suggest that weight loss interventions may be able to reduce the risk of AF [Mahajan R et al. Heart Lung Circ 2013]. This hypothesis has also been tested in a small randomized clinical trial in which 150 obese patients with symptomatic AF were randomly assigned to no treatment (n=75) or to a dietary intervention intended to achieve a 10% weight reduction (n=75) [Abed HS et al. JAMA 2013]. The dietary intervention was successful in reducing waist circumference and BMI. AF symptom scores, indicative of symptom burden and severity, were also reduced for patients who were randomly assigned to the dietary intervention (Figure 2).

Atrial Fibrillation Symptom Scores
Reproduced from Abed HS et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA 2013;310(19):2050–2060. © 2013 American Medical Association. All rights reserved.

The editors would like to thank the many members of the 2014 Heart Rhythm Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
The possible benefits of a weight reduction program for outpatients with AF was investigated in the Aggressive Risk Factor Reduction Study—Implications for AF study [ARREST-AF; Pathak RK et al. HRS 2014 (AB31–06)], with the hypothesis that late recurrence of AF after AF ablation reflects progression of the underlying conditions. In the study, 149 consecutive patients undergoing their first AF ablation chose a risk factor management strategy (n=61), whereas the other patients did not (n=88). AF recurrence was assessed in both groups (who were similar at baseline in a battery of relevant characteristics) during the ongoing follow-up. AF-free survival was significantly better in the risk-managed patients treated once or more for AF.
These data support the hypothesis that obesity is a modifiable risk factor influencing the burden of AF.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.