

Summary
The clinical implications of atrial tachycardia (AT) and atrial fibrillation (AF) episodes <5 minutes in duration are unknown. Such episodes can be detected with implanted cardiac rhythm management (CRM) devices. The aim of the prospective Registry of Atrial Tachycardia and Atrial Fibrillation Episodes in the Cardiac Rhythm Management Device Population [RATE; NCT00837798] was to document the incidence of AT and AF, along with associated clinical data, in a large group of patients with implanted pacemakers or implantable cardioverter-defibrillators.
- Arrhythmias
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
The clinical implications of atrial tachycardia (AT) and atrial fibrillation (AF) episodes <5 minutes in duration are unknown. Such episodes can be detected with implanted cardiac rhythm management (CRM) devices. The aim of the prospective Registry of Atrial Tachycardia and Atrial Fibrillation Episodes in the Cardiac Rhythm Management Device Population [RATE; NCT00837798] presented by Michael V. Orlov, St Elizabeth's Medical Center, Brighton, Massachusetts, USA, was to document the incidence of AT and AF, along with associated clinical data, in a large group of patients with implanted pacemakers (PMs) or implantable cardioverter-defibrillators (ICDs). The investigators hypothesized that short AT or AF episodes in the RATE population would be associated with prespecified clinical adverse events (AEs) and confer a high risk of subsequent longer episodes of AT or AF.
In total 5379 patients receiving new PMs (n=3141) or ICDs (n=2238) without documented AF in the previous 3 months were enrolled at 225 sites in the United States. Device and AE data were analyzed every 6 months during the 2-year follow-up. All hospitalizations, emergency department visits, and in-hospital deaths were adjudicated by 8 teams of 2 physicians blinded to the electrogram (EGM) data. Because there were an estimated 13,000 EGMs, a random sample and a case-control sample were adjudicated. The random sample consisted of randomly selected patients, with a sample size sufficient to provide 95% confidence of defining the true incidence of AT and AF. All EGMs from 300 patients with a PM and 300 patients with an ICD were included in the random sample. The case-control sample consisted of all EGMs from all patients with AEs (cases); 2 controls were matched to each case.
The registry was conducted from 2007 to 2012, and the median follow-up was 23 months. In the random sample, the total incidence of AT and AF was 48% in the PM group (40% long duration and 9% short duration) and 52% in the ICD group (36% long duration and 16% short duration). In the case-control sample, the total incidence of AT and AF was ∼40% in the cases and ∼30% in the controls (Table 1).
Incidence of Atrial Tachycardia and Fibrillation
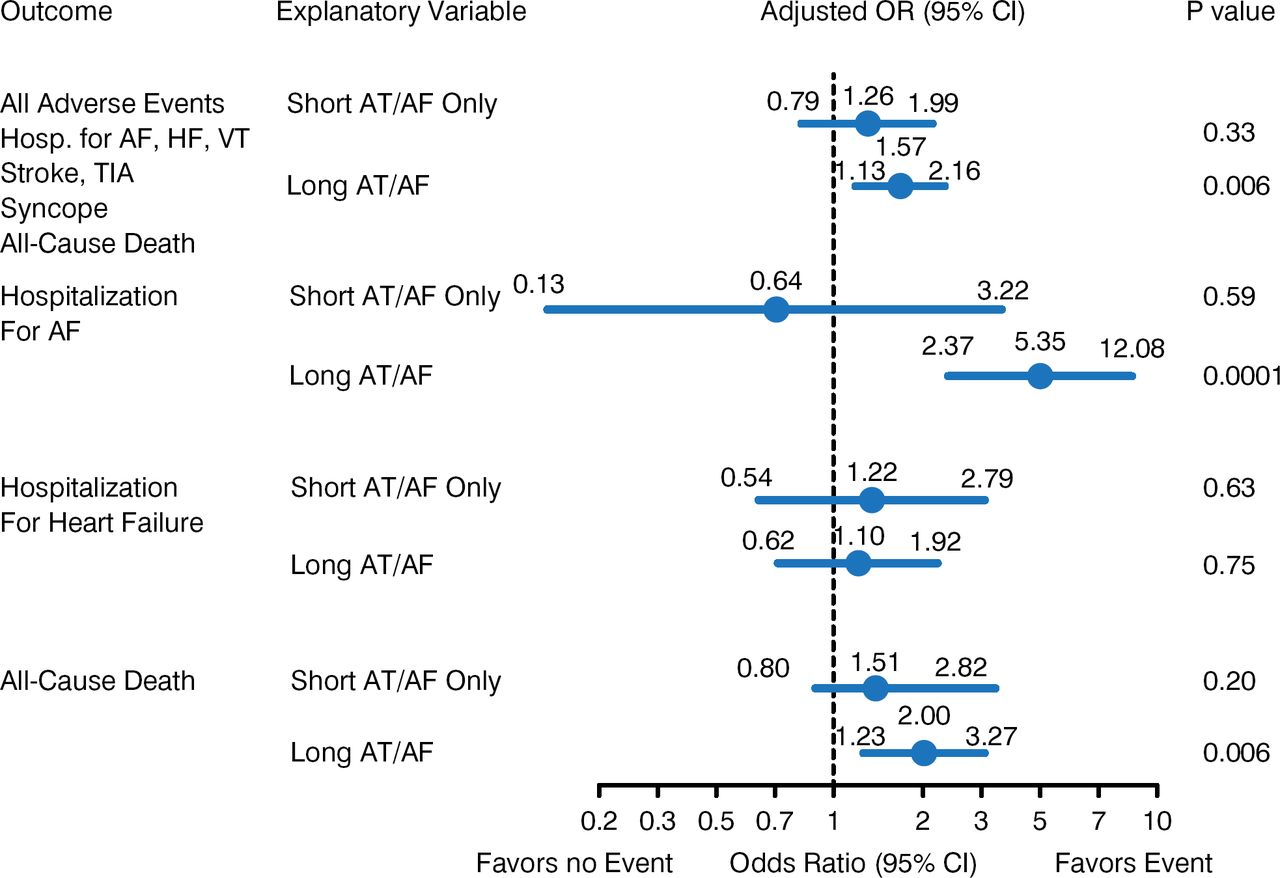
AEs included 118 hospitalizations and 191 deaths in the PM group and 290 hospitalizations and 168 deaths in the ICD group. Long AT or AF episodes were associated with all AEs in the ICD group (p=0.006), including hospitalization for clinical AT or AF (p=0.0001) and all-cause death (p=0.006; Figure 1). There was no significant association between AT or AF episodes and AEs in the PM group. Patients with only short AT or AF episodes were not at a higher risk of AEs than were those without AT or AF during follow-up.

Rates of Clinical Events, AT, and AF in the ICD Groupa
AF=atrial fibrillation; AT=atrial tachycardia; EF=ejection fraction; HF=heart failure; Hosp=hospitalization; ICD=implantable cardioverter-defibrillator; MI=myocardial infarction; TIA=transient ischemic attack; VT=ventricular tachycardia.
a Adjusted ORs include covariates: anticoagulant (crude OR 1.7 for all events), hypertension (OR 1.4), prior stroke (OR 1.2), prior VT (OR 1.3), prior MI (OR 1.2), EF (OR 1.2 per 10% reduction).
Occurrence of short AT or AF was significantly associated with development of long AT or AF over time in ICD patients (HR, 1.54; p=0.04) but not in PM patients (HR, 1.35; p=0.20).
AT or AF was documented in half the CRM population within 2 years. Approximately 1 in 4 of these patients had only short AT or AF episodes. Patients with long AT and AF episodes in the ICD group had more AEs, including hospitalization and all-cause death. Dr. Orlov concluded that many patients with short AT or AF episodes will not develop long AT or AF episodes within a 24-month period.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.