

Summary
This article discusses the latest guidelines for the treatment of hypertension in patients with dyslipidemia, diabetes, atrial fibrillation, and chronic kidney disease.
- Hypertensive Disease
- Diabetes & Kidney Disease
- Arrhythmias
- Lipid Disorders
- Cardiology Guidelines
- Renal Disease
- Diabetes Mellitus
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
- Diabetes & Kidney Disease
- Arrhythmias
- Lipid Disorders
- Cardiology Guidelines
- Renal Disease
- Diabetes Mellitus
This session focused on the latest guidelines for the treatment of hypertension in patients with dyslipidemia, diabetes, atrial fibrillation (AF), and chronic kidney disease (CKD).
2013 AMERICAN COLLEGE OF CARDIOLOGY /AMERICAN HEART ASSOCIATION GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL
Genovefa Kolovou, PhD, Onassis Cardiac Surgery Center, Athens, Greece, provided an overview of the American College of Cardiology/American Heart Association 2013 guidelines on the treatment of blood cholesterol [Stone NJ et al. Circulation 2013], highlighting changes in the recommendations since the previous version.
Dr. Kolovou stressed that these guidelines address treatments proved to reduce atherosclerotic cardiovascular disease (ASCVD) events and are not intended to be a comprehensive approach to lipid management. The updates in the new guidelines focus on identifying individuals most likely to benefit from statin therapy and clarify treatment goals for lowering low-density lipoprotein cholesterol (Table 1).
ACC/AHA 2013 Guideline Updatesa
The new guidelines identify high-, moderate-, and low-intensity statins for use in the secondary and the primary prevention of ASCVD (Table 2).
High-, Moderate-, and Low-Intensity Statin Therapya
Dr. Kolovou concluded that ASCVD is the most important public health problem of our time. Achieving consistency of clinical care, incorporating new evidence, and its synthesis into practical recommendations for clinicians is the task of various guideline committees throughout the world. According to Dr. Kolovou, the guidelines could be enhanced by refining the use of lipid goals rather than by removing them.
HYPERTENSION MANAGEMENT AND GLYCEMIC CONTROL IN DIABETES
Peter M. Nillson, MD, PhD, Skane University Hospital, Malmo, Sweden, discussed guidelines for blood pressure (BP) and glycemic control in patients with diabetes. The goals of antihypertensive therapy in patients with diabetes are to lower BP and reduce cardiovascular risk and mortality.
Both the European guidelines on cardiovascular disease prevention [Perk J et al. Eur Heart J 2012] and the American Diabetes Association (ADA) Standards of Medical Care in Diabetes 2014 [ADA. Diabetes Care 2014] recommend a hypertension treatment target in patients with diabetes of <140/80 mm Hg. The 2013 European Society of Hypertension (ESH)/European Society of Cardiology (ESC) recommendations [Mancia et al. Eur Heart J 2013] are shown in Table 3.
ESH/ESC Guidelines for the Treatment of Hypertension in Diabetes and Metabolic Syndrome
The ESC/European Association for the Study of Diabetes and ESH/ESC guidelines both suggest that combination therapy is often necessary for patients with diabetes and hypertension. When combination therapy is needed, an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB), calcium antagonist, and thiazide diuretic are recommended. The guideline cautions against using an ACE inhibitor plus an ARB or a direct renin inhibitor because of the adverse effects of acute kidney injury and hyperkalemia. Beta-blockers should be used in patients with concomitant symptomatic coronary heart disease. Thiazides and beta-blockers may increase the risk for new-onset diabetes.
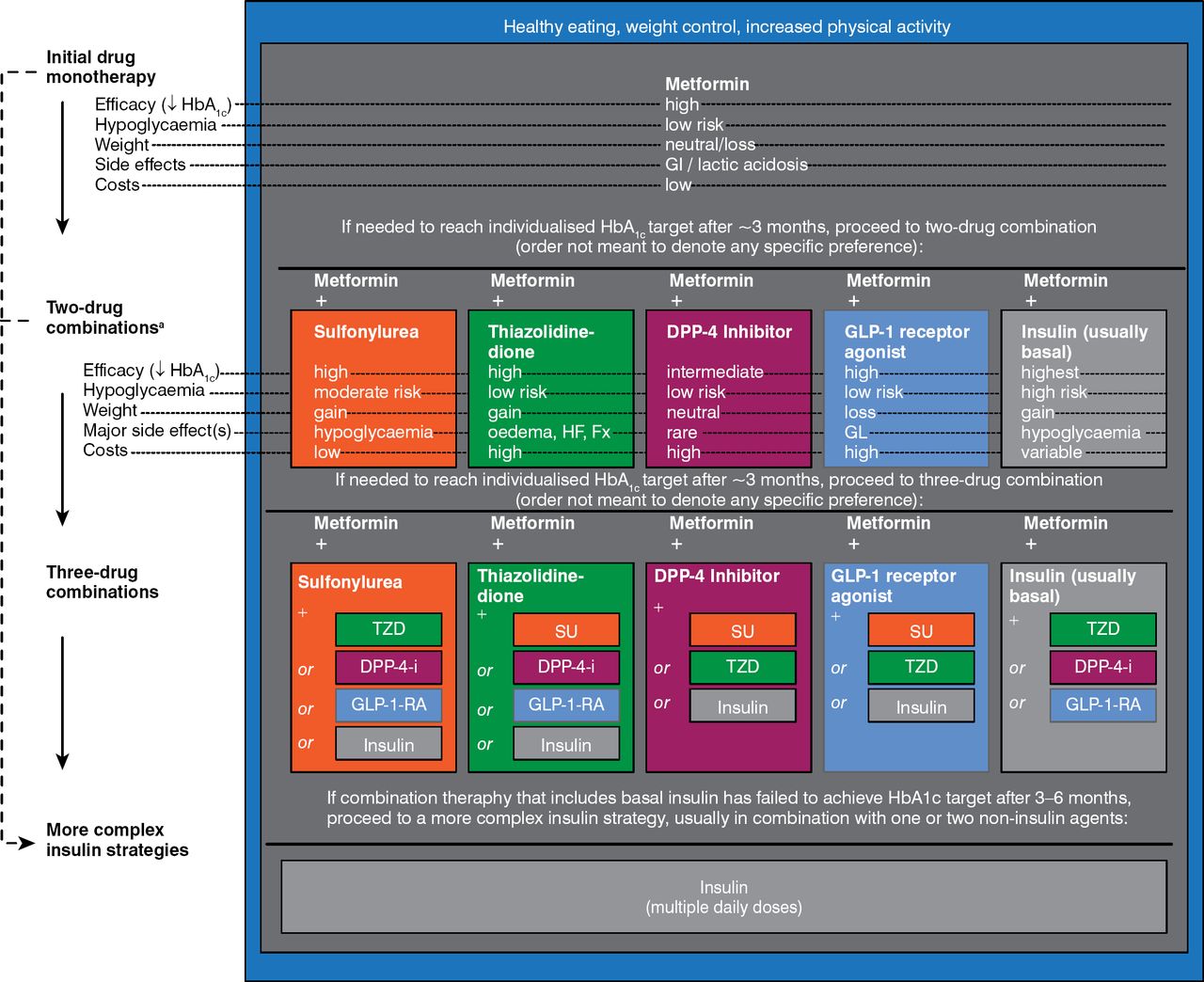
The ADA/European Association for the Study of Diabetes (EASD) 2012 guidelines for glycemic control [Inzucchi SE et al. Diabetologia 2012] in patients with diabetes recommend initial drug monotherapy with metformin in addition to lifestyle changes. More advanced regimens should use multiple glucose-lowering drugs, possibly insulin (including greater than once daily injections; Figure 1). Glycated hemoglobin (HbA1C) targets may need to be adjusted to avoid hypoglycemia.

ADA/EASD Guidelines for Glycemic Control in Patients With Type 2 Diabetes
ADA=American Diabetes Association; DPP=dipeptidyl peptidase; EASD=European Association for the Study of Diabetes; GI=gastrointestinal; GLP=glucagon-like peptide; HbA1C= glycated hemoglobin; SU=sulfonylurea; TZD=thiazolidinedione.
Reproduced with permission from Springer Verlag from Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55(6):1577–1596.
Flexible goals for controlling hypertension (<140/85 mm Hg) and hyperglycemia (<7% HbA1C) are now recommended to avoid adverse effects, especially in the frail elderly (<8%–9% HbA1C). The ADA's BP goal for patients with diabetes, now <140/80 mm Hg, has gradually changed to become more like the European goal. The ESH/ESC and ESC/EASD 2013 guidelines both recommend a BP goal of <140/85 mm Hg, but the International Society of Hypertension/American Society of Hypertension recommend a goal of <140/90 mm Hg.
THERAPY FOR PATIENTS WITH ATRIAL FIBRILLATION AND HYPERTENSION
Patients with hypertension have an increased risk for AF, which leads to reduced cardiac function and increased risk for thromboembolism. Enrico Agabiti Rosei, MD, University of Brescia, Italy, discussed the various guidelines for antihypertensive, antiarrhythmic, and antithrombotic therapy for patients with AF.
The 2013 ESH/ESC guidelines for the management of arterial hypertension recommend considering treatment with an ARB, an ACE inhibitor, a beta-blocker, or a mineralocorticoid receptor antagonist to prevent AF and a beta-blocker or nondihydropyridine calcium antagonist for ventricular rate control in hypertensive patients with AF [Mancia et al. Eur Heart J 2013]. The 2012 focused update of the ESC guidelines [Camm AJ et al. Eur Heart J 2012] recommends antiarrhythmic therapy according to underlying pathology. Patients with AF have a nearly 5-fold increased risk for stroke [Wolf PA et al. Stroke 1991]. A meta-analysis found that two-thirds of strokes due to AF are preventable with appropriate anticoagulant therapy; in 29 trials of 28,044 patients, adjusted-dose warfarin reduced ischemic stroke by 67% and all-cause mortality by 26% [Hart RG et al. Ann Intern Med 2007]. The new oral anticoagulants (NOACs), dabigatran, rivaroxaban, apixaban, and edoxaban have been evaluated for stroke prevention in several trials. A meta-analysis of randomized clinical trials comparing NOACs with warfarin reported a 19% overall reduction in stroke risk and a 14% overall reduction in major bleeding risk with NOACs versus warfarin [Ruff CT et al. Lancet 2014].
The ESC AF 2012 [Camm AJ et al. Eur Heart J 2012] and AHA/ACC/Heart Rhythm Society 2014 [January CT et al. Circulation 2014] guidelines for the treatment of AF recommend warfarin, dabigatran, rivaroxaban, or apixaban in patients with CHA2DS2VASc scores ≥2. The American College of Chest Physicians 2012 guidelines [Guyatt GH et al. Chest 2012] recommend dabigatran 150 mg twice daily rather than vitamin K antagonist therapy, while the Canadian Cardiovascular Society AF guidelines [Skanes AC et al. Can J Cardiol 2012] recommend dabigatran, rivaroxaban, or apixaban over warfarin (Table 4).
US, European, and Canadian Guidelines for the Management of Patients With Atrial Hypertension
According to Prof. Agabiti Rosei, prevention of AF and new treatment regimens are needed, considering the increasing elderly population, high percentage of uncontrolled hypertension, risk for stroke, and worsening of other comorbidities. Management of AF includes antihypertensive, antiarrhythmic, and antithrombotic drugs. Prof. Agabiti Rosei also emphasized that most patients with hypertension and AF do not control BP adequately, and this might represent a risk for cerebral hemorrhage, particularly during anticoagulant therapy.
TREATMENT OF HYPERTENSION IN PATIENTS WITH KIDNEY DISEASE
The latest guidelines for the treatment of hypertension in patients with CKD were discussed by Demetrios V. Vlahakos, MD, Attikon University Hospital, Athens, Greece. According to the 2013 ESH/ESC guidelines for the management of arterial hypertension, patients with CKD and hypertension have a high to very high risk for cardiovascular disease [Mancia et al. Eur Heart J 2013]. For patients with CKD stage 3 or ≥4, the guidelines recommend lifestyle changes for those with high normal BP (systolic BP [SBP] 130–139 mm Hg or diastolic BP [DBP] 85–89 mm Hg) and lifestyle changes plus antihypertensive therapy targeting a BP <140/90 mm Hg for patients with hypertension (SBP ≥140 mm Hg or DBP ≥90 mm Hg).
A meta-analysis studying the effects of intensive BP lowering on the progression of kidney disease reported that intensive BP therapy improved outcomes and reduced the risk for end-stage kidney disease [Lv J et al. CMAJ 2013]. Subgroup analysis showed that intensive BP lowering reduced the risk for kidney failure for patients with baseline proteinuria but not for those without proteinuria.
BP-lowering therapies recommended by the 2013 ESH/ESC guidelines are shown in Table 5.
Hypertension Treatment for Patients With Nephropathy
The 2014 evidence-based guideline for the management of high blood pressure in adults recommends that antihypertensive therapy in adults with CKD include an ACE inhibitor or ARB to improve kidney outcomes [James PA et al. JAMA 2014].
Prof. Vlahakos concluded that guidelines provide evidence-based recommendations for the thresholds, goals, and drug treatment strategies for the management of hypertension. However, guidelines are not a substitute for clinical judgment, and decisions must carefully consider the specific characteristics of each patient.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.