

Summary
This article highlights select advances in the management of cardiovascular disease risk. It discusses personalized medicine in the management of cardiovascular disease, the role of e-cigarettes in smoking cessation and reduction, and the Global Cardiovascular Nursing Leadership Forum in mobilizing nurse leaders to promote prevention of cardiovascular disease worldwide.
- cardiovascular disease
- e-cigarettes
- GCNLF
- nurses
- PCNA
- personalized medicine
- smoking
- stroke
- vaping
- genomics
- smoking cessation
A panel of speakers discussed recent improvements and innovations that could advance the field of cardiovascular disease (CVD) prevention and significantly improve public health.
Personalized Medicine in CVD
Personalized medicine (PM) is about moving away from a “one-size-fits-all” approach to health care, said Mary Kerins, RGN, MSc, St James’ Hospital, Dublin, Ireland. This form of medicine uses the science of genomics and proteomics and provides the means to predict, prevent, treat, and cure disease, as well as to enable targeted diagnoses, prognoses, and therapies to promote individual wellness and advance health care.
Despite the significant progress of PM since its introduction in the late 1990s, including in the field of CVD, Kerins emphasized that CVD remains the leading cause of mortality in women, and it accounts for 30% of deaths globally and 40% of deaths in the European Union (EU). Although PM is playing a growing role in health care, she noted that it remains in development in the EU, and she highlighted key findings from a report released in 2012 from the European Hospital and Healthcare Federation (HOPE) and PricewaterhouseCoopers (PwC) that discussed movement toward PM in 6 European hospitals [HOPE, PwC. Personalised Medicine in European Hospitals. 2011].
The report documented that most European hospitals focused on initiatives related to diagnostics and therapeutics. Wide use of genetic screening was found in cancer treatment. In contrast, however, stem cell programs were rarely used, and telemedicine is not yet fully implemented. In addition, most hospitals did not address disease prevention, and only a few focused on nutrition and exercise to encourage wellness and enhance patient treatment. The major barriers to implementation of PM were found to be a lack of the following:
Research funding
Robust scientific evidence in some fields
Doctors’ knowledge about PM
A clear reimbursement system for related services
Nevertheless, these findings merely emphasize the opportunity for hospitals to adapt this novel model of health care to individual patient-targeted services, said Kerins. However, she stressed the need to design and implement PM according to an individual hospital’s needs, organization, and operational pattern.
In her closing remarks, Kerins noted that it takes about 17 years for clinical research findings to be implemented routinely into clinical practice, and she stressed the need for a multidisciplinary approach to PM, as well as more research and regulation in this area. Although medicine of the past focused on population medicine, medicine of the future will focus on an individual, she concluded.
e-Cigarettes: Harmful or Helpful?
According to Peter Hajek, MA, PhD, Queen Mary University of London, London, United Kingdom, e-cigarettes (ECs) could represent a revolutionary development to improve the health of smokers.
He noted that the main components of the liquid in ECs are propylene glycol, vegetable glycerol, nicotine, and flavorings. And, although they contain potential toxicants, the concentrations of these substances are much lower than in smoke (< 1%) and are unlikely to pose serious risks to health. In addition, passive exposure to ECs is unlikely to be harmful, he added.
Nevertheless, controversy has clouded the debate over ECs and tobacco control, in particular due to concern that they represent a gateway to smoking for children or nonsmokers. However, Prof Hajek stressed that research has shown that up to now, ECs have not been impeding the decline in smoking and may even be helping it. Vaping has also been estimated to carry < 5% of the risk of smoking. Consequently, there is a need to correct the public’s misperceptions of the risks of ECs, he said.
Prof Hajek shared data from a Cochrane Review of studies involving ECs, emphasizing the absence of either serious adverse events or safety concerns associated with vaping over the short to medium term (up to 2 years) [McRobbie H et al. Cochrane Database Syst Rev. 2014].
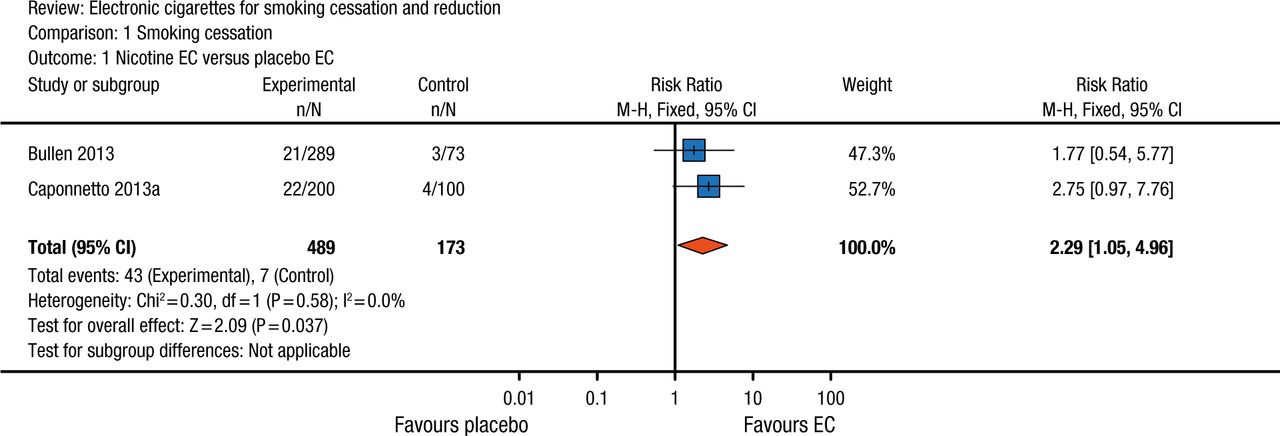
In fact, data from this review suggested that ECs help smokers to quit smoking (Figure 1). In those who do not quit, they may reduce the quantity of smoking. But Prof Hajek noted that the review was based on a small number of studies and that further studies are needed to confirm this finding.
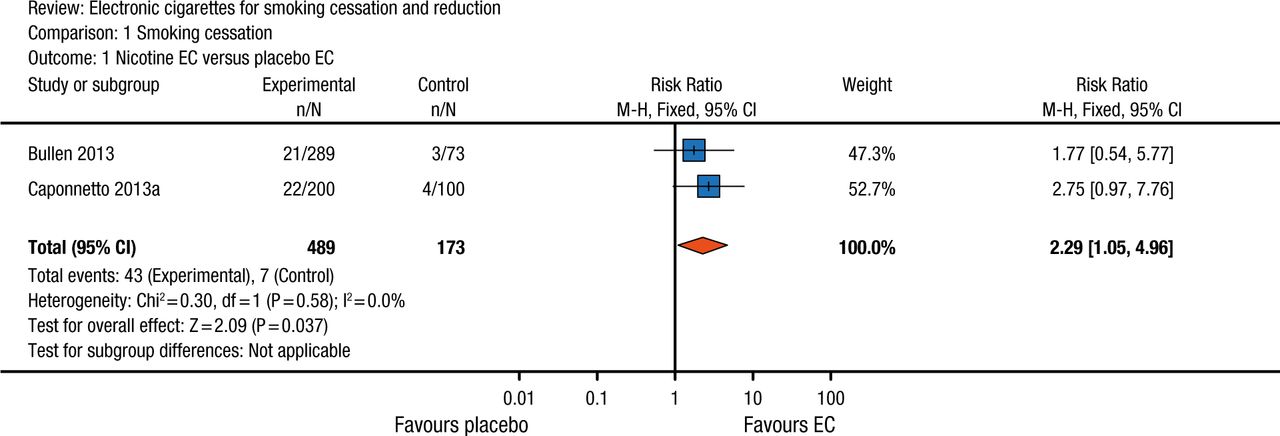
The Efficacy of e-Cigarettes on Smoking Cessation
df, degrees of freedom; EC, electronic cigarette; M-H, Mantel-Haenszel method for calculating risk ratio.
Reprinted from McRobbie H et al, Electronic cigarettes for smoking cessation and reduction, Cochrane Database Syst Rev, Vol 12; CD010216, Copyright © (2014), with permission from The Cochrane Collaboration.
Overall, however, based on current evidence, smokers who switch to ECs reduce their health risks significantly. And there is no evidence that ECs are enticing children to start vaping or smoking, said Prof Hajek. Nevertheless, ongoing surveillance is important to monitor for potential emergence of new risks and enable regulations to be revised accordingly. Public health priorities should aim to encourage smokers to switch from smoking to vaping. Provided they are not impeded by excessive regulation, ECs could make smoking obsolete, concluded Prof Hajek.
The Global Cardiovascular Nursing Leadership Forum
Barbara J. Fletcher, RN, MN, University of North Florida and Mayo Clinic Florida, Jacksonville, Florida, USA, discussed the Global Cardiovascular Nursing Leadership Forum (GCNLF), a Preventive Cardiovascular Nurses Association–initiated strategic plan.
Because 12 million nurses comprise the largest health care discipline managing CVD risk, Fletcher noted that the American Heart Association and World Health Organization recognize the pivotal role that nurses play in the goal to reduce CVD deaths by 25% by 2025 [Hayman LL et al. J Am Coll Cardiol. 2015]. According to Fletcher, the mission of the GCNLF is to engage and mobilize an international community of nurse leaders to promote prevention of CVD and stroke worldwide.
Following the inaugural meeting of the GCNLF in 2014, findings demonstrated
A lack of standardization of nursing curricula
lack of outcomes data demonstrating that nurses influence CVD care
A lack of reimbursement for nurse-based prevention
The perception of CVD prevention as a nonpriority
In addition, barriers to nurses’ continuity of care included
Short patient hospital stays
Nurses being too busy
Nurses’ lack of awareness about prevention
Lack of follow-up
Variation in technological support
Substantial educational and clinical practice gaps in CVD prevention were also found, both between and within countries. Consequently, the GCNLF aims to address these findings, said Fletcher, and to promote collaboration with other health care providers and international organizations dedicated to the prevention of CVD and stroke. Its next steps involve development of a website with access to educational resources on CVD and evidence-based guidelines. The GCNLF is also compiling a plan for international nursing organizations to determine how nurses can be more effective in global CVD and stroke prevention, concluded Fletcher.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.