

Summary
According to the US Centers for Disease Control and Prevention, the 2014 Ebola outbreak in West Africa is the largest Ebola outbreak in history and the first to be classified as an epidemic. This article reviews the clinical characteristics of patients infected with Ebola, as well as reviews the global response in tracking and managing the outbreak and provided an overview of potential therapeutic options.
- Viral Infections
- Screening & Prevention
- Viral Infections
- Screening & Prevention
According to the US Centers for Disease Control and Prevention (CDC), the 2014 Ebola outbreak in West Africa is the largest Ebola outbreak in history and the first to be classified as an epidemic. As of September 25, 2014, > 6200 cases had been reported, with Liberia and Sierra Leone accounting for > 83% of the cases [CDC, September 25, 2014]. At the time of the 2014 Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC), no cases had been reported in the United States except for four patients who contracted the disease in West Africa and were transferred emergently to the United States.
To address this critical public health issue, three speakers discussed various aspects of the epidemic. Barbara Knust, DVM, PMH, CDC, Atlanta, Georgia, USA, began by presenting basic facts about the virus itself. Ebola is a zoonotic virus of the Filoviridae family that is transmitted from infected animals to humans or nonhuman primates, and is taken over by human-human transmission. The virus is not transmitted through the air; rather, it is transmitted by direct contact with body fluids from a symptomatic, infected person or animal, or an object contaminated with infected body fluids (ie, syringe).
Dr Knust reviewed the clinical characteristics of patients infected with Ebola, which typically starts as a nonspecific, flu-like febrile illness (Table 1). After a few days, however, the predominant clinical syndrome is a severe gastrointestinal illness with vomiting and diarrhea. Volume depletion with a range of metabolic disorders ensues, and hypovolemic shock ultimately occurs. Because no approved therapies currently exist, early intervention and supportive care are the mainstays of treatment [Clark DV et al. Viruses. 2012].
Clinical Presentation of Patients with the Ebola Virus
Although symptoms may appear anywhere from 2 to 21 days after initial exposure, the average onset is 8 to 10 days. According to Dr Knust, the most important effort in stopping the West African outbreak has been to admit those identified in the early stages of the disease to a designated “Ebola treatment center.” This requires effective diagnostic screening in the field or a regional laboratory to differentiate between patients infected with Ebola and other tropical diseases such as malaria and typhoid fever that do not require the same rigorous control measures. It is also important to find the patient's close contacts and follow them for 21 days, because they are the next likely to develop the disease.
After reviewing the epidemiologic pattern of the virus throughout West Africa since March 2014, Dr Knust reviewed the barriers to containing the outbreak. The primary reasons are due to the high level of mobility across the borders in this geographic area as well as a general mistrust of interventions implemented by the government. Another important challenge is the resistance of the local populations to abandon ritual burial practices, which include holding and bathing the corpse. Dead bodies infected with Ebola carry a high level of the virus in body fluids and on the skin, which puts loved ones at risk. There are also insufficient numbers of healthcare workers, medical supplies, and personal protective equipment (PPE). At the time of the ICAAC presentation, there had been > 260 healthcare workers diagnosed with Ebola, typically related to a lack of PPE, insufficient training, and sanitary measures.
Dr Knust closed her talk with a list of CDC activities related to this Ebola outbreak. These activities include data management, contact tracing and case finding, health education, infection control, laboratory diagnosis support, and coordination with other responding agencies. She emphasized the importance of reinforcing efforts to implement infection control methods and safer burial practices to prevent this outbreak from advancing to a humanitarian crisis and an overall collapse of the healthcare system in West Africa.
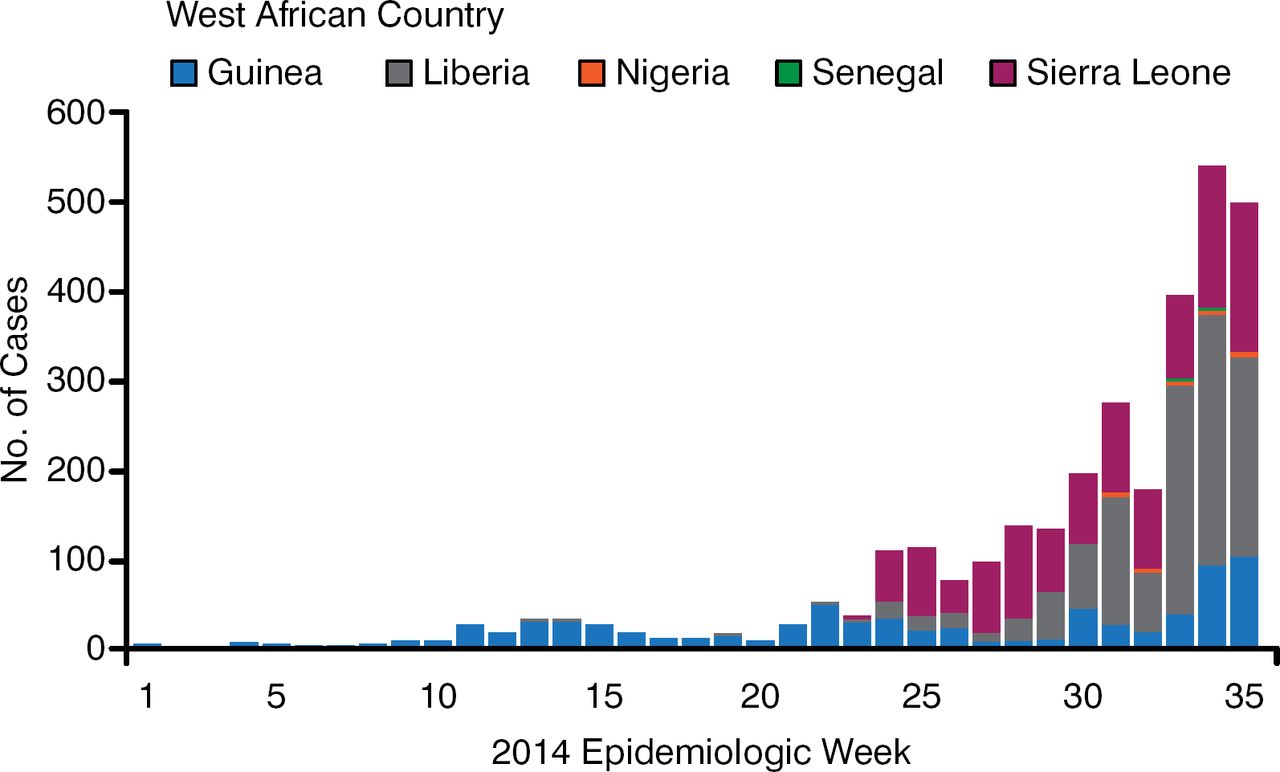
Gary Kobinger, PhD, National Microbiology Laboratory, Winnipeg, Manitoba, Canada, reviewed the global response in tracking and managing the outbreak and provided an overview of potential therapeutic options. He first showed epidemiologic data demonstrating that after an initial downturn in cases reported in Guinea, two subsequent outbreaks occurred—a trend never previously observed (Figure 1).

West Africa Combined Epidemiologic Curves, Weeks 1–35
Source: World Health Organization, September 5, 2014.
Dr Kobinger also described the work of 7 field laboratories in breaking the chain of Ebola transmission. Symptomatic patients are brought onsite to a treatment center where a PCR-based, rapid diagnostic test is performed. This differentiates among patients that harbor the Ebola virus vs other agents that cause similar symptoms such as malaria, cholera, or Lassa fever. Patients with Ebola can then be positively identified and managed accordingly. The goal of the field laboratories is to identify the causative agent within 3 hours from receipt of the sample.
Dr Kobinger went on to discuss the future of therapeutic options to treat Ebola. One option continues to be the use of convalescent plasma from patients recovering from the infection; this strategy has been effective in treating other viruses, including H1N1 influenza [Hung IF. Clin Inf Dis. 2011]. Based on work with nonhuman primates, monoclonal antibodies (mAbs) appear to be another promising option. Among 21 critically ill macaques infected with Ebola, all 18 who received 3 doses of mAbs (ZMapp) cleared the virus from the circulation when given the drug within 5 days of the viral challenge. The three animals that did not receive the drug died [Qiu X et al. Nature. 2014]. At the time of the ICAAC presentation, this treatment had been provided to 7 patients during this outbreak, although the treatment is not currently approved anywhere in the world for commercial use. Two of these patients have died. Dr Kobinger also reviewed several other therapeutics and vaccines under development.
Aneesh Mehta, MD, Emory University Hospital, Atlanta, Georgia, USA, then spoke of his perspectives as a member of the team caring for two American patients who had been infected with Ebola in Liberia and subsequently admitted to Emory University Hospital in August 2014 by air ambulance. He reviewed lessons learned in five areas—clinical care of patients, laboratory testing and diagnostics, staff and environmental safety, waste management, and communications management.
Dr Mehta described the layout of the hospital's serious communicable diseases (SCD) unit, which includes dedicated laboratory space, isolated patient rooms with private baths, and separate staff shower and changing rooms. He emphasized that while a dedicated laboratory is not required to care for patients with SCDs, such a facility does allow for immediate results and less impact among hospital and laboratory staff [Hill CE et al. Lab Med 2014].
Dr Mehta then described the CDC recommendations for taking precautions to prevent transmission of the Ebola virus (CDC. Ebola Virus Disease 2014). These include recommendations regarding the necessity of placing patients in single rooms with private baths; using disposable medical equipment when possible; the proper use of PPE, including gloves, gowns, eye protection, face-masks, and disposable shoe coverings; management of aerosol-generating procedures; and monitoring of potentially exposed personnel. The CDC has also issued interim guidance for environmental infection control related to patients who have Ebola virus (Table 2).
Environmental Infection Control for Hospitals Treating Patients With Suspected or Confirmed Ebola Virus
In addition to the clinical and environmental considerations, Dr Mehta emphasized the importance of implementing a coordinated operations and communications effort that keeps all stakeholders apprised of events prior to or as they occur. This would include hospital administration and personnel; local, state, and federal government agencies; service providers; and the media. According to Dr Mehta, the primary goal of these communication efforts is to assure all stakeholders that (1) the hospital has expertise in serious infectious diseases, (2) the staff is trained and prepared to care for these patients, and (3) the hospital will protect its patients, staff, and communities at all costs.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.