

Summary
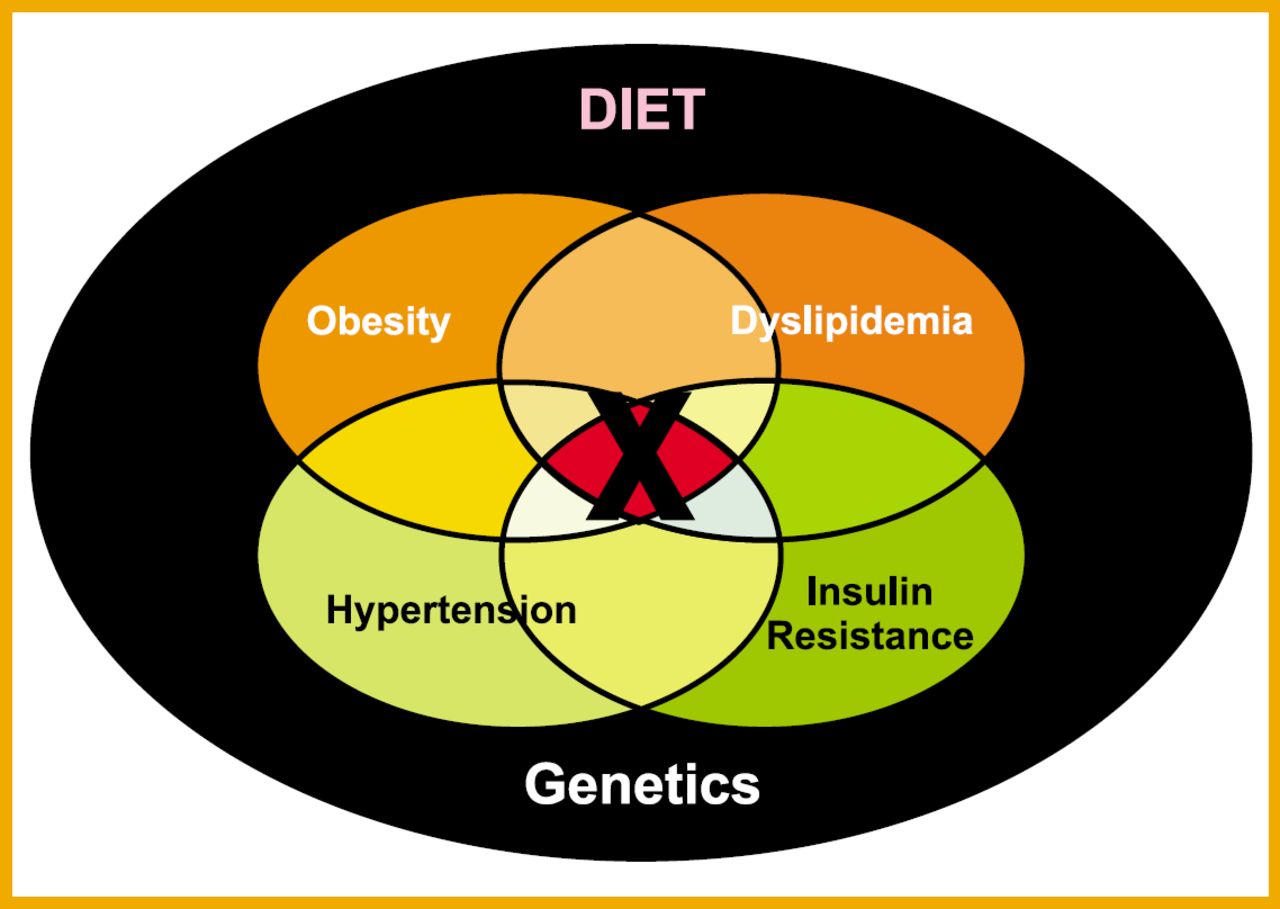
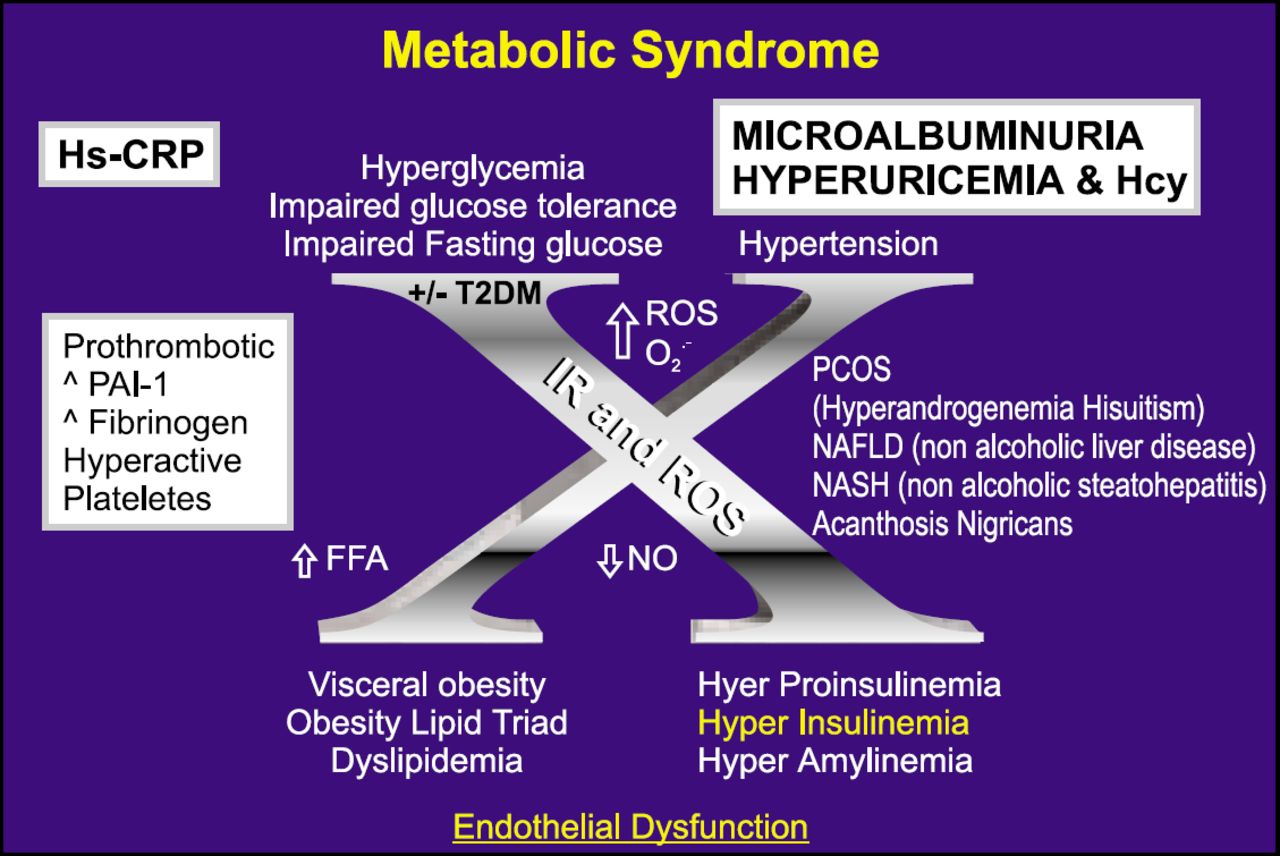
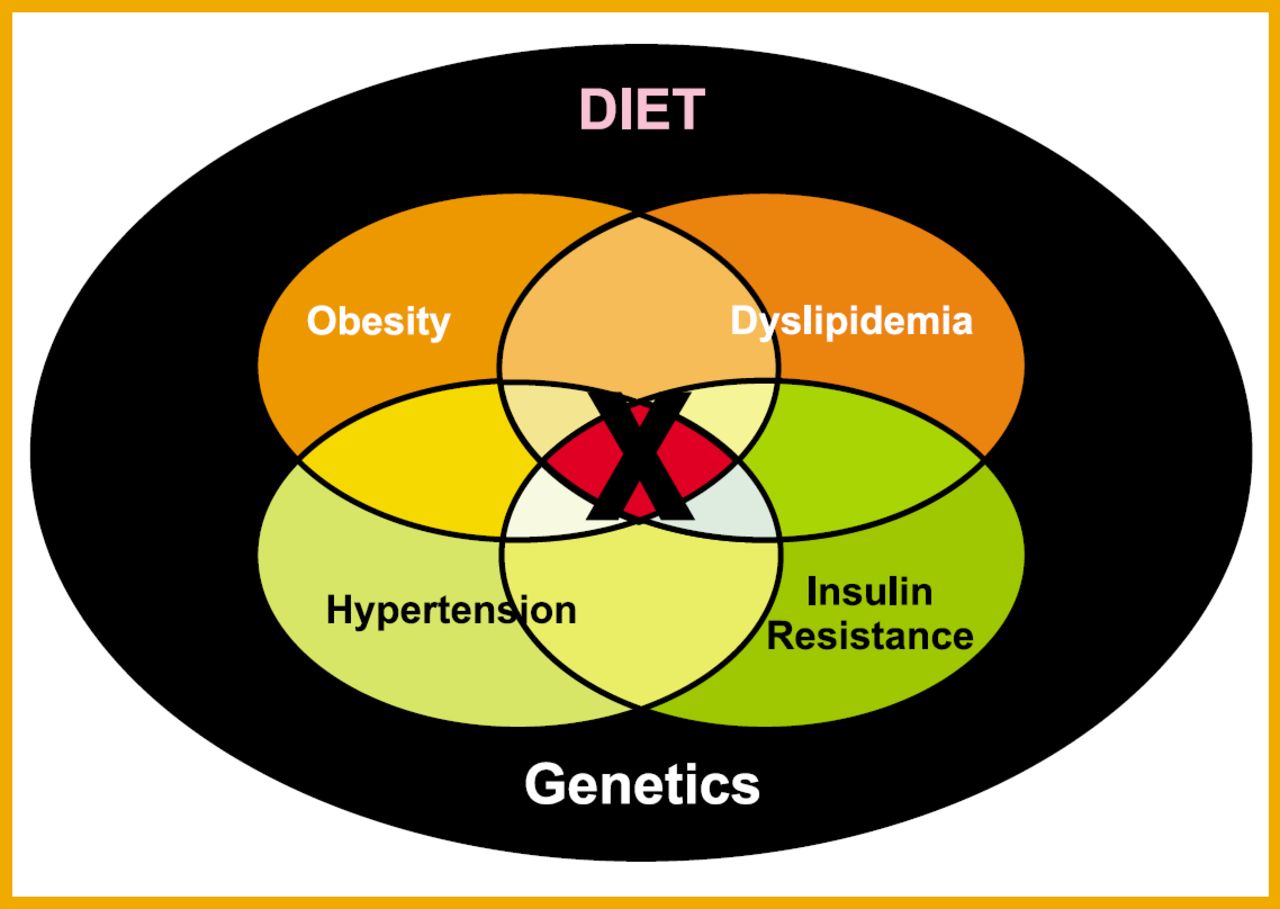
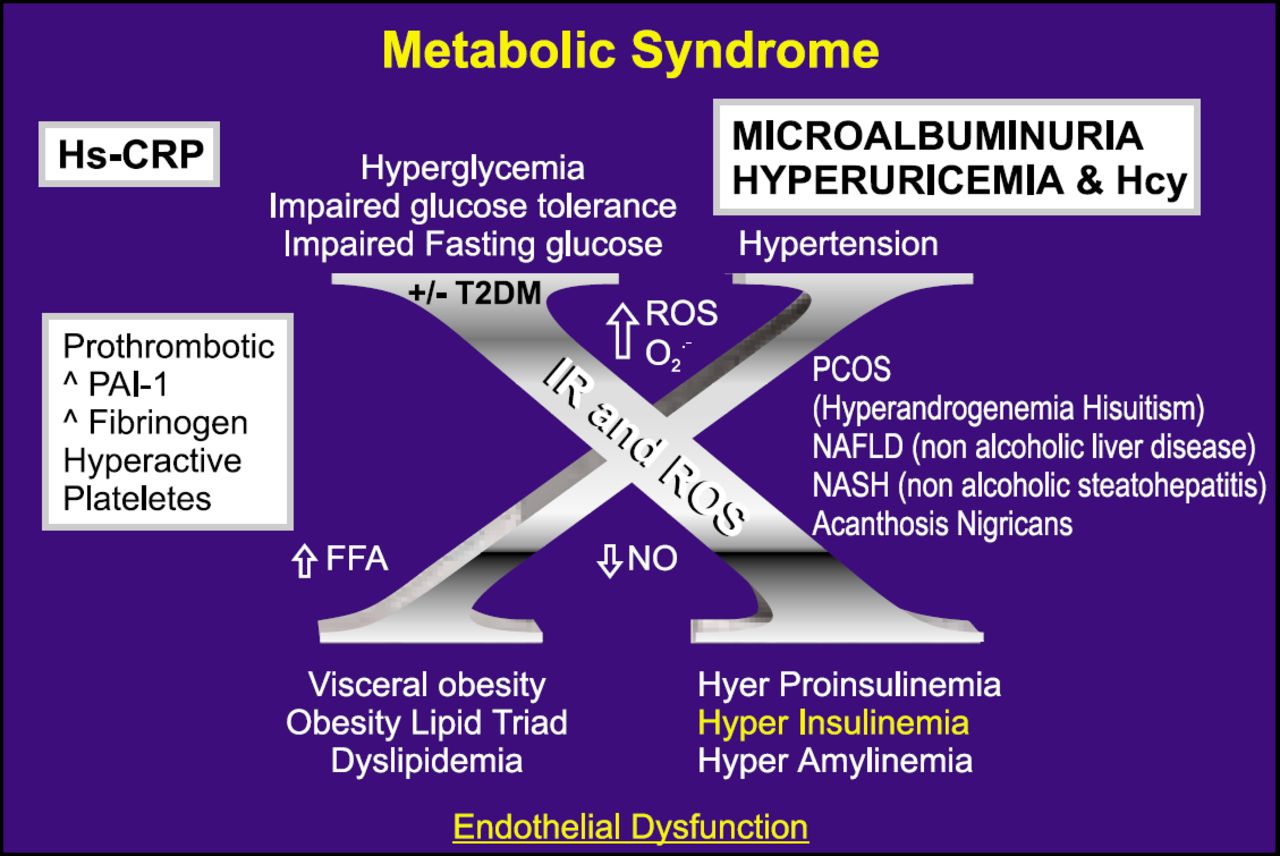
What was once known as “Syndrome X” has grown into a clinical entity known as Metabolic Syndrome (MetS). Now understood to be a complex interaction of several metabolic variables that, in combination, exacerbate hypertension, coronary artery disease, and diabetes, MetS is one of the most important health burdens in the developed world. As research progresses, metabolic syndrome appears to have biochemical and causal relationships with many unexpected abnormalities (asthma, gout, polycystic ovary disease) as well as with behavioral conditions such as depression and chronic hostility and anger.
- cardiometabolic
- Cardiometabolic
- polycistic ovary (Diabetes)
What was once known as “Syndrome X” has grown into a clinical entity known as Metabolic Syndrome (MetS). Now understood to be a complex interaction of several metabolic variables that, in combination, exacerbate hypertension, coronary artery disease, and diabetes, MetS is one of the most important health burdens in the developed world. As research progresses, metabolic syndrome appears to have biochemical and causal relationships with many unexpected abnormalities (asthma, gout, polycystic ovary disease) as well as with behavioral conditions such as depression and chronic hostility and anger.
MetS: Synergy of Components or Syndrome?
“Research on metabolic syndrome (MetS) has seen enormous growth in the last few years,” said David C. Goff, Jr., MD, PhD, co-director of the Center for Health Care Research and Quality and a professor of Public Health Sciences and Internal Medicine at the Wake Forest University School of Medicine in Winston-Salem, NC.
Although MetS now has its own journal, Metabolic Syndrome and Related Disorders, and a recent PubMed search for MetS yielded nearly 15,000 citations, Dr. Goff observed that “we are still not certain MetS is actually a syndrome.” Pointing to several papers including an October 2005 position paper sponsored by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), Dr. Goff acknowledged that some researchers believe MetS does not yet meet the formal definition of a syndrome.
“Some of our colleagues maintain that MetS is a ‘synergy of components’ rather than a true syndrome,” Dr. Goff said. But the fact remains that “the existing data makes it clear the converging elements of MetS help to identify individuals at high risk for cardiovascular disease (CVD) and type 2 diabetes (T2DM).” Whether these factors collaborate to exacerbate the various conditions associated with MetS, or exist in tandem as independent risk factors, Dr. Goff noted that “studies generally agree there is a stepwise increase of risk” as each additional element of MetS is identified in a patient.
MetS is recognized as significant risk predictor of CHD, and is now thought to be an expression of genetic phenotype exacerbated by behavioral factors—sedentary lifestyle, smoking, and being either overweight or obese. As new data accumulates, other conditions have been linked to MetS, not only biochemical factors such as oxidative stress, inflammation, and autonomic dysregulation, but depressive symptoms and negative affective states including chronic anger, hostility, and mood disorders.
“There is clearly more going on with MetS than simply the sum of its parts,” Dr. Goff said. “And it seems clear, whether we call it a syndrome or simply a connected set of conditions, MetS is going to become an ever more challenging problem.”
Physical Activity and Metabolic Syndrome
Gerald Fletcher, MD, of the Mayo Clinic in Jacksonville, FL, offered a keynote presentation on MetS and exercise. “Physical activity is absolutely critical in primary prevention,” Dr. Fletcher said. “The aspects of MetS impacted by exercise include blood pressure, elevated triglycerides, low HDL, and glucose tolerance. And the data is unequivocal: exercise reduces MetS, reduces risk, and limits cardiovascular events.”
Dr. Fletcher reported that average blood pressure reductions of 2.4 mm/Hg (systolic) and 5.8 mm/Hg (diastolic) were observed across several recent studies of exercise and metabolism. In citing other recent data published in Circulation (LaMonte MJ et al. CIRC 2005; 112:505–512), he noted that decreased cardiorespiratory fitness is strongly associated with MetS, saying that “low cardiorespiratory fitness is a strong and independent predictor of MetS in both women and men.”
The best exercise programs combine moderate intensity and endurance, and should be an activity that a patient can live with for the rest of their life. “It's best to recommend varied intensity in any single exercise session,” Dr. Fletcher said. “The key is consistency and regularity rather than exercising to exhaustion 1 or 2 days a week.” Dr. Fletcher's official advice: 30–60 minutes of moderate intensity exercise “on most days” for weight control and maintenance of target weight. Patients should be cautioned to avoid more than 2–3 weeks of “exercise abstinence,” as it takes up to 6 weeks to re-condition to prior levels after 2–3 weeks of no activity.
Ultimately, Dr. Fletcher said that “patients must be encouraged to assume responsibility and physicians must serve as examples and champions for exercise. We all just need to move more and do more.”
Psychological and Novel Risk Factors
As research continues, MetS has been linked to depression, sleep apnea, asthma, polycystic ovary syndrome, gestational diabetes, and gout.
Some researchers have postulated the existence of a “vascular depression,” where depression is more difficult to treat in the presence of CAD. According to Viola Vaccarino, MD, PhD, Associate Professor at Emory University School of Medicine in Atlanta, GA, depression affected neurohormonal pathways contribute to a “stress cascade,” driving cortisol levels above baseline and furthering changes that predispose to diabetes, sodium retention, hypertension, as well as the truncal adiposity associated with dyslipidemia and MetS.
Dr. Vaccarino reported findings of her study of 281 male twins born from 1945–1955. Study data yielded a correlation between major depression (at least 1 incident) and subsequent development of MetS—a connection that appears to be independent of behavioral and environmental factors. Dr. Vaccarino postulated that depression and mood disorders may be linked to the development of MetS and increased CAD risk through stress-induced neuroendocrine pathways.
Mercedes Carnethon, PhD, professor of preventive medicine at Northwestern University in Chicago, IL, discussed novel risk factors that appear to enhance development of MetS, including sleep disturbances (insomnia, sleep apnea), and behavioral factors such as depression, anxiety, and hostility. Dr. Carnethon also reviewed recent studies that link inflammation and endothelial dysfunction, diabetes, depression, MetS, and CAD risk.
Dr. Carnethon noted that smoking—a major risk factor for both MetS and CAD—is associated with insulin resistance. “We are dealing with a constellation of factors involving both physiological and behavioral elements,” she said. “We have seen evidence that both oxidative stress and autonomic dysfunction contribute to MetS as well as depression and anxiety. More research is needed to help us understand how to intervene in this complex problem.”
Is There a Rational Drug Therapy Treatment for MetS?
According to Alan Chait, MD, Professor of Medicine and Head, Division of Metabolism, Endocrinology and Nutrition at the University of Washington, Seattle, the components of MetS are treated independently. “The ideal treatment for metabolic syndrome will be to treat the syndrome at the biochemical source and block all downstream manifestations. This is where we need to go in the future. This is where our research needs to point.”
Chait acknowledged that “TLC” (therapeutic lifestyle changes) is always the first step in managing a patient with one or more elements of MetS. But all too often TLC fails to arrest dyslipidemia, hypertension, and impaired fasting glucose. Chait focused on the dyslipidemic aspects of MetS, referring to the HDL-Atherosclerosis Treatment Study (HATS), which assessed a combination of simvastatin plus niacin in 160 patients with documented CAD and low HDL levels. Nearly half of the study participants had MetS based on NCEP ATP III criteria. In those participants with MetS, the simvastatin + niacin treatment led to 40% reduction in CAD events and 90% reduction in coronary artery stenosis. (Brown BG et al. N Engl J Med. 2001; 345: 1583–92.)
Dr. Chait reviewed considerations for treatment of dyslipidemias, particularly the combination of elevated triglyceride (TG) and lowered HDL that marks MetS. Since statins tend to have a lesser effect on TG and HDL, niacin or fibrates used in combination with a statin may be indicated.
In general, Dr. Chait noted that “atorvastatin in combination with fibrates offer excellent outcomes” in patients with MetS. “But the ideal treatment - one we hope our research takes us toward - will treat the cause of MetS, not the expressions. Until then, we must aggressively treat all modifiable risk factors for this condition.”
- © 2005 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.