

Summary
Epidemiologic data have shown that a Mediterranean diet that is low in saturated fat and high in polyunsaturated fats reduces low-density lipoprotein cholesterol and lowers the risk of cardiovascular events. Yet, the clinical evidence of benefit with the components of these diets is mixed, and are reviewed in this article. Other topics include reshaping nutrition habits in clinical practice, as well as a review on epidemiological and clinical evidence of the negative impact of sugar-sweetened beverages on health.
- Cardiometabolic Disorder
- Prevention & Screening
- Nutrition Physiology
- Obesity
- Assessment
- Cardiometabolic Disorder
- Prevention & Screening
- Endocrinology
- Diabetes & Metabolic Syndrome
- Nutrition Physiology
- Obesity
- Assessment
Epidemiologic data have shown that a Mediterranean diet that is low in saturated fat and high in polyunsaturated fats reduces low-density lipoprotein cholesterol and lowers the risk of cardiovascular events. Yet, the clinical evidence of benefit with the components of these diets is mixed, and was reviewed by Peter Clifton, MBBS, University of South Australia, Adelaide, Australia.
The Mediterranean diet recommends a low intake of saturated fats and high monounsaturated fats, with a low intake of meat and dairy, and high intake of fruits, vegetables, legumes, and nuts. Alcohol intake is modest.
Prof. Clifton discussed numerous studies that showed benefit of the Mediterranean diet and its components. Frequent nut consumption (>5 times/week) was associated with a 35% reduction in the incidence of coronary heart disease (CHD) in 4 epidemiological studies [Kris Etherton et al. J Nutr 2008]. In addition, a Mediterranean diet supplemented with extra virgin olive oil or nuts was associated with lower risk of CV events in the Prevención con Dieta Mediterránea (PREDIMED; Table 1) study [Estruch R et al. N Engl J Med 2013].
PREDIMED
In the EPIC-NL cohort study of nearly 35,000 middle-aged persons without known CVD, a significant protective effect was found for each 2-point increment in the Mediterranean-style diet [Hoevenaar-Blom MP et al. PLoS One 2012]. The Spanish EPIC study showed that each 10 gram increase in olive oil consumption was associated with a 7% reduction in CHD [Buckland G et al. Br J Nutr 2012]. The Greek EPIC study found that each 2-unit increase in the Mediterranean diet score was associated with a 16% reduction in total mortality [Trichopoulou A et al. BMJ 2009].
Fruits and vegetables have been found to be associated with the same level of benefit in epidemiologic trials and are recommended as part of the DASH (Dietary Approaches to Stop Hypertension) diet for lowering blood pressure. However, there are no prospective clinical data showing that fruit and vegetable intake reduces CV events. Fish has been found to be associated with benefits in studies conducted in the United States, but this association has been less strong in Scandinavian studies. Recent intervention studies with fish oil have not found them to reduce CV events [The ORIGIN Trial Investigators. N Engl J Med 2012; de Caterina R et al. N Engl J Med 2011]. Meat and dairy products appear to be neutral or have mildly positive effects (dairy only). More data are required to identify the optimal level of salt intake. Some data have shown that limiting its intake is associated with a reduction in stroke and CV disease; however, increased salt intake can increase heart failure and may increase CV events in patients with diabetes.
RESHAPING NUTRITION HABITS IN CLINICAL PRACTICE
The public knows that a healthy diet is important for disease prevention, yet they are confused by the many different messages and changing research claims, said Benoît Lamarche, PhD, Université Laval, Québec City, Québec, Canada. Restrictive diets are difficult to sustain long-term and usually are most effective when coupled with support, which is usually short-term.
The 2010 United States Department of Agriculture dietary recommendations were useful because they moved from nutrient-based recommendations to food-based recommendations. More effective than restricting foods is adding foods or nutritional components that may be beneficial. This approach was studied in the PREDIMED study which showed the primary composite endpoint of myocardial infarction (MI), stroke, and CV death was reduced with the Mediterranean diet supplemented with extra virgin olive oil (HR, 0.70; 95% CI, 0.53 to 0.91; p=0.009) and with nuts (HR, 0.70; 95% CI, 0.53 to 0.94; p=0.02) [Estruch R et al. N Engl J Med, 2013].
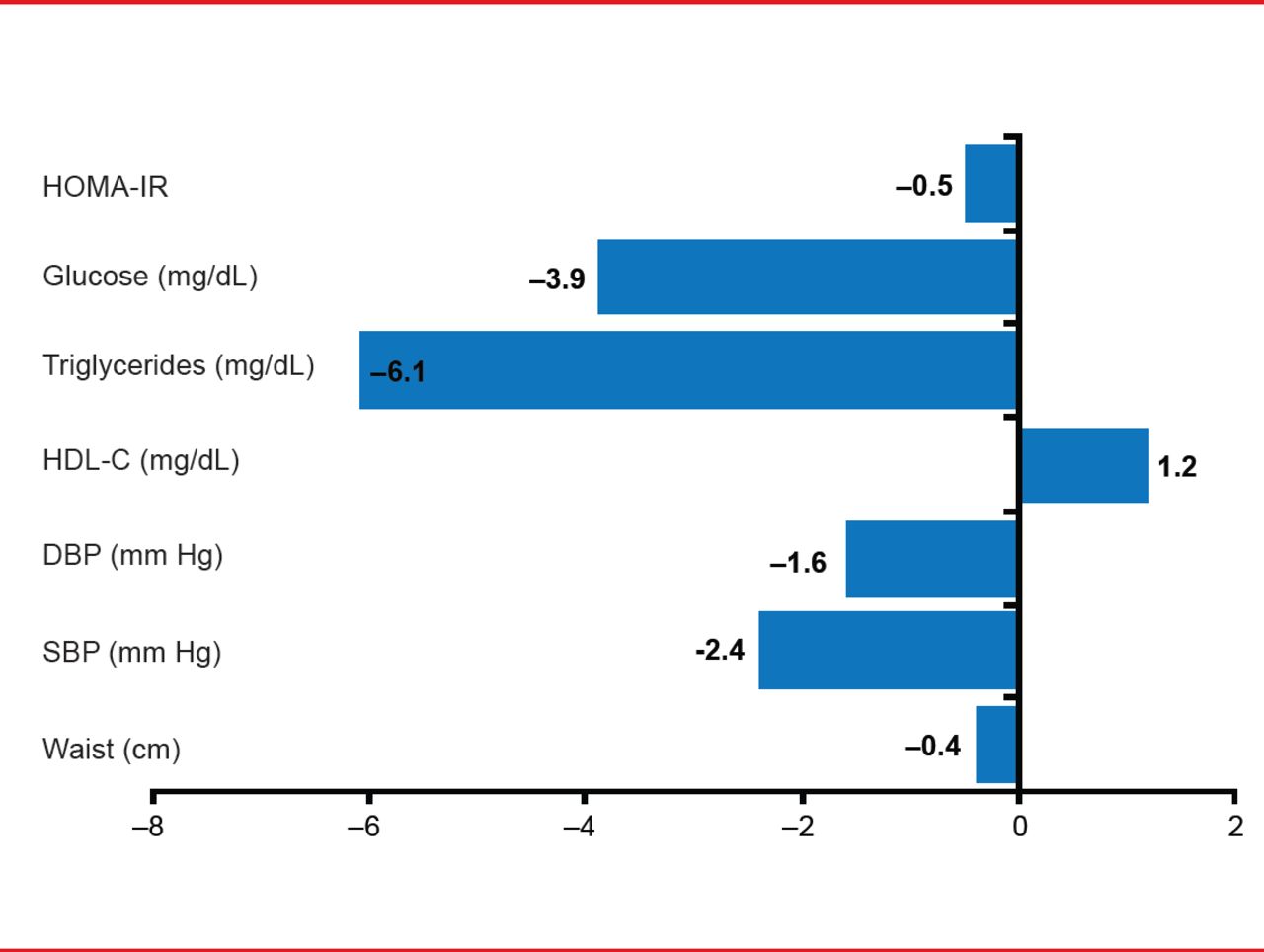
A recent meta-analysis showed the Mediterranean diet is associated with positive effects (to different degrees) on metabolic syndrome and its components (Figure 2) [Kastorini CM et al. J Am Coll Cardiol 2011].

Effect of Mediterranean Diet on Metabolic Syndrome and Its Components in Meta-Analysis
DBP=diastolic blood pressure; HDL-C=high-density lipoprotein cholesterol; HOMA-IR=homeostatic model assessment of insulin resistance; SBP=systolic blood pressure; TG=triglycerides.
Reproduced from Kastorini CM et al. The Effect of Mediterranean Diet on Metabolic Syndrome and its Components: A Meta-Analysis of 50 Studies and 534,906 Individuals. J Am Coll Cardiol 2011;57(11):1299–1313. With permission from Elsevier.
A series of studies by Richard, Lamarche, and colleagues have shown that the Mediterranean diet has beneficial effects whether or not patients also lose weight. LDL-C was reduced by 9.9% along with a significant reduction in plasma PCSK9 (by 11.7%; p<0.01) and the phytosterol:cholesterol ratio (by 9.7%; p<0.01) versus control diet, with no additional benefit with weight loss [Richard C et al. Br J Nutr 2012]. They also showed that adipokines were not reduced in patients who did not lose weight with the Mediterranean diet [Richard C et al. Metabolism 2013]. Inflammation was also reduced with the Mediterranean diet regardless of weight loss, as measured by C-reactive protein (CRP), interleukins, and other measures, and greater reductions in waist circumference in men were associated with greater reductions in inflammatory markers [Richard C et al. Obesity (Silver Spring) 2013].
HEALTH CONSEQUENCES OF SUGAR-SWEETENED BEVERAGE CONSUMPTION
Frank B. Hu, MD, PhD, Harvard School of Public Health, Boston, Massachusetts, USA, reviewed epidemiological and clinical evidence of the negative impact of sugar-sweetened beverages (SSBs) on health. Although consumption of SSBs has plateaued in the United States over the last decade, consumption has skyrocketed globally, and SSB consumption patterns can make huge differences in weight gain, he said.
SSBs contain 3.1 to 3.6 grams of sugar per ounce, or about 10 teaspoons per 12-ounce can. They are sweetened with high fructose corn syrup. SSB consumption patterns predicted weight gain in an epidemiological study of the effects of SSBs in a cohort of children [Ludwig DS et al. Lancet 2001].
The most rigorous trial of SSBs showed replacing high-caloric with noncaloric drinks reduced weight gain and fat accumulation in normal-weight children [de Ruyter JC et al. N Engl J Med 2012]. A meta-analysis of 11 studies with nearly 311,000 participants showed that SSBs were associated with an increased risk of type 2 diabetes (RR, 1.26; 95% CI, 1.12 to 1.41) and increased risk of metabolic syndrome (RR, 1.20; 95% CI, 1.02 to 1.42) in the higher quartiles of SSB consumption compared with the lower quartiles [Malik VS et al. Diabetes Care 2010].
High consumption of SSBs is linked to several health risks, including increased body weight, diabetes, CVD, metabolic syndrome, and gout. Dr. Hu recommended more sugar-free or low-sugar alternatives be made available and that strategies learned from fighting tobacco abuse be used to reduce the consumption of SSBs. He proposed a multipronged approach that includes education, regulation, and taxation. The Obesity Prevention Source (www.obesitypreventionsource.org) provides information and materials to educate children.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.