

Summary
While human leukocyte antigen (HLA) matched sibling stem cell transplantation can eradicate chemotherapy-resistant leukemia, only 30% of patients are fortunate enough to have such a match. Therefore, studies began determining if HLA unrelated adult volunteer donors could provide an effective source of allogenic stem cells.
- Oncology Genomics
- Leukemia
While human leukocyte antigen (HLA) matched sibling stem cell transplantation can eradicate chemotherapy-resistant leukemia, only 30% of patients are fortunate enough to have such a match. Therefore, studies began determining if HLA unrelated adult volunteer donors could provide an effective source of allogenic stem cells.
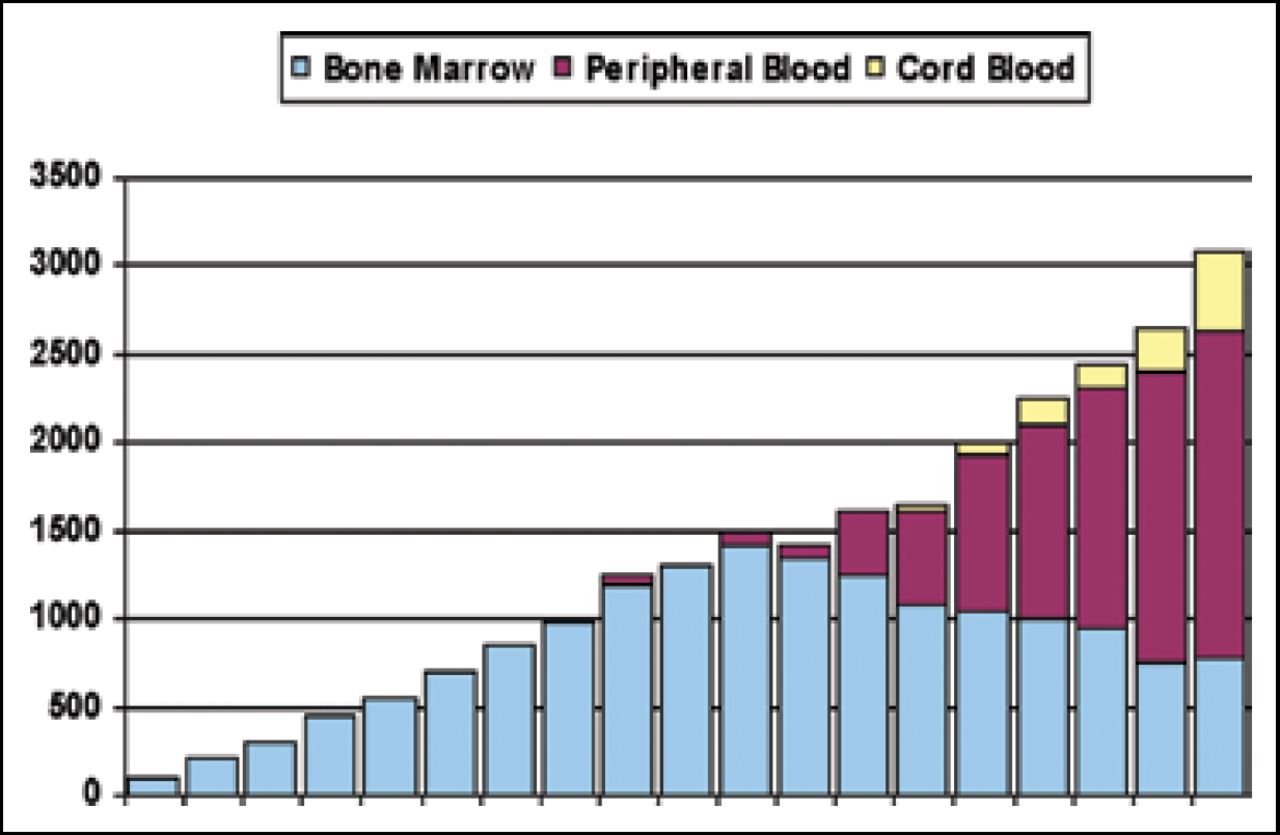
Given the large number of polymorphisms in the HLA gene, however, the probability of finding two matched individuals is low, necessitating a registry with millions of donors. With a concerted effort over the last fifteen years, the donor registry has grown to approximately six million donors in the US. These donors provide various sources of stem cells for transplantation, including bone marrow, which dominated from 1988–2000, peripheral blood stem cells (PBSCs), which comprised a large part of transplants from 2001 until the present, and recently, cord blood (Figure 1).
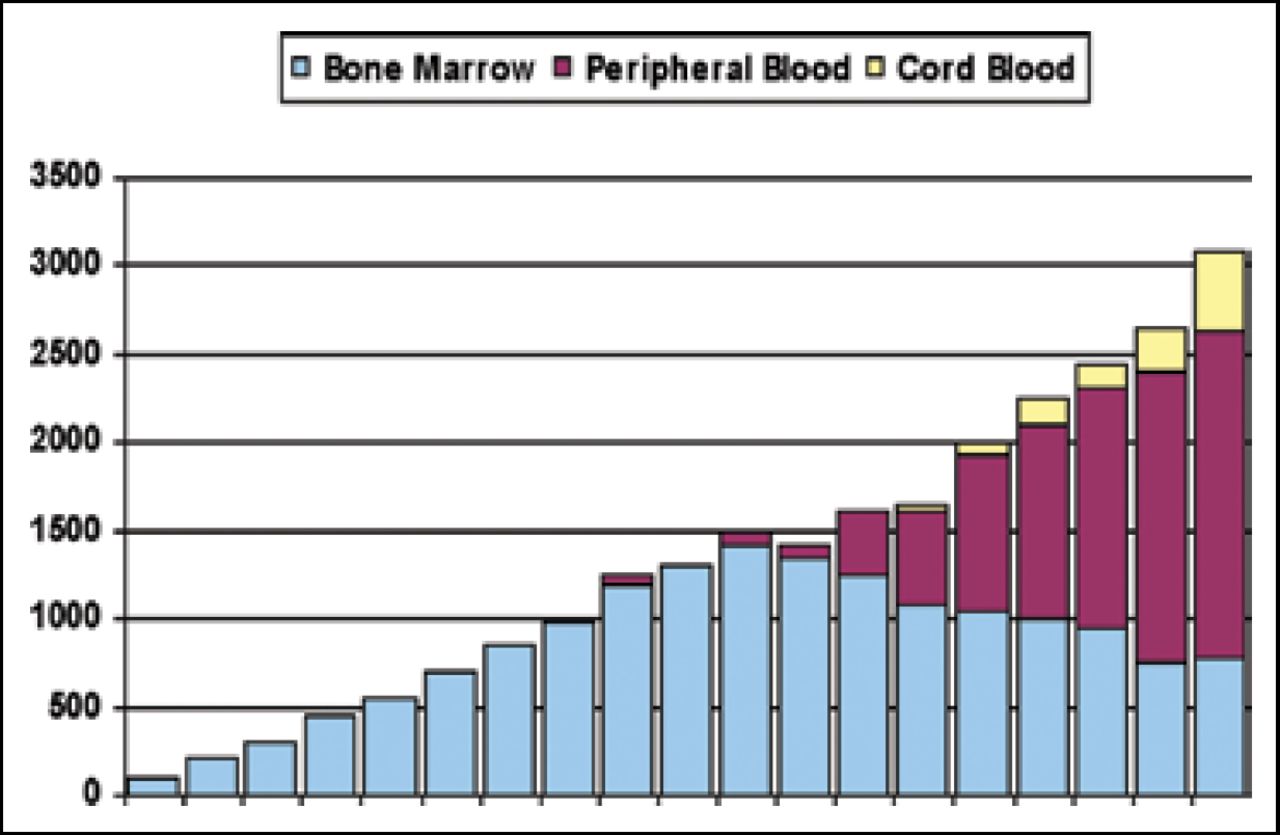
Unrelated Stem Cell Sources Over the Past Two Decades.
Stem cell therapy (SCT) is indicated for a variety of syndromes. Acute myeloid leukemia (AML) is the biggest indicator for an allogenic stem cell transplant, followed by acute lymphoblastic leukemia (ALL), myelodysplastic syndromes (MDS), lymphoma and chronic myelogenous leukemia (CML). A recent study [Tallman et al. Blood 2007] showed that survival of patients with AML harboring unfavorable cytogenetics appears to be at least as good as that for matched sibling transplants, and better than consolidation chemotherapy. The authors concluded from this that AML patients in CR1 with unfavorable cytogenetics and without a matched sibling should be offered unrelated donor transplants.
For CML, studies have shown that survival is better in patients with low and intermediate-1 disease when donor transplantation is performed at progression, whereas survival is better with intermediate-2 and advanced disease when transplant is immediate [Cutler C. Blood 2004]. For ALL, the majority of patients receiving unrelated donor stem cells are CR1 and about 40% of them enjoy long-term survival. CML patients generally receive allogenic transplantation in the chronic phase.
Donor Selection
It has been shown that loci HLA-A, -B and DR are important for the overall success of transplantation, though other loci have been explored recently. Indeed, data published in 2004 showed that HLA-C is as important as HLA-A and -B for survival [Flomenberg et al. Blood 2004]. A mismatch in any of these loci is significantly associated with a plethora of adverse events [Lee et al. ASH 2006] (Table 1). Matching these important loci, however, is associated with the best survival and deferring the use of a mismatch donor should be weighed against the risk of progressive disease. Additionally, recent changes in donor search algorithms allow more precise, efficient and rapid searches.
Relative Risk of Adverse Event with Any Single HLA Mismatch.
Stem Cell Sources
The dose of CD34 cells achieved in SCT is associated with a better outcome; PBSCs contain more CD34 cells than bone marrow (BM), thus the rationale for using mobilized blood rather than marrow. However, a retrospective comparison of PBSC vs BM transplantation showed that the increase in graft-versus-host-disease (GVHD) associated with PBSC transplantation results in similar overall survival rates for the two stem cell sources. A randomized clinical trial is required to help define the role of peripheral blood grafts.
Development of Reduced Intensity Regimes
Reduced intensities of chemotherapeutic regimes can extend allogenic transplant options to older patients. One study showed that replacing the standard busulfan/cyclophosphamide with busulfan/fludaribine resulted in higher rates of event-free survival with decreased toxicity [Russel JA et al. Biol Blood Marrow Transplant 2002; de Lima M et al. Blood 2004; Field T et al. Blood 2006]. However, controlling GVHD remains a challenge; GVHD prophylaxis can be effective in this case.
Umbilical Cord Blood in Transplant Medicine
“Just a few years ago, it [umbilical cord blood] was considered a biological waste,” remarked John Wagner, MD, Stem Cell Institute of the University of Minnesota, when emphasizing the progress that has been made in this area to date. As of May 29th, 2007, roughly 8,000 umbilical cord blood transplants (UCBT) had been performed.
The reasons to explore the use of UCB as a source of stem cells are compelling. Transplant-related mortality, whether using marrow or blood, is approximately 45% after three years. These suboptimal survival rates are due partly to the incidence of adverse events, such as high regimen-related toxicities, high risks of acute and chronic GVHD and slow immune responses. The aim is to find a stem cell source, or a new approach, that decreases the risk of opportunistic infections.
The unique properties of UCB, such as decreased cyctotoxicity, increased proportion of regulatory T cells, circulating trophoblasts that secrete high levels of IL-10, altered cytokine profiles that may result in less GVHD, has prompted much interest in this new source. The Cord Blood Transplant Study (COBLT) was the first prospective, multicenter trial to look at UCB in transplantation [Cornetta K et al. Biol Blood Marrow Transplant 2005]. This study determined that cell dose is critical for engraftment, GVHD is low despite significant HLA mismatches, and survival is comparable to that observed in marrow recipients despite HLA mismatch.
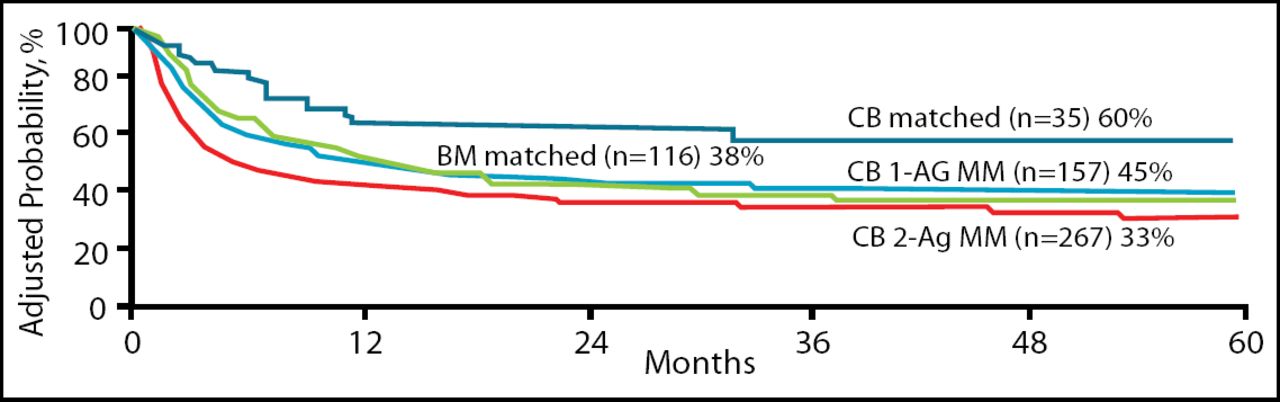
A retrospective study compared UCBT to the standard-of-care allele matched BM from adult unrelated donors [Eagen M et al. In press 2007]. This study showed that patients receiving cord blood (CB), whether matched or mismatched, experienced a significantly lower rate of acute or chronic GVHD than those who received marrow. Even more encouraging is that patients receiving matched cord blood had better overall survival rates than those receiving matched BM; also, unmatched CB had overlapping survival rates to those of matched BM (Figure 2).
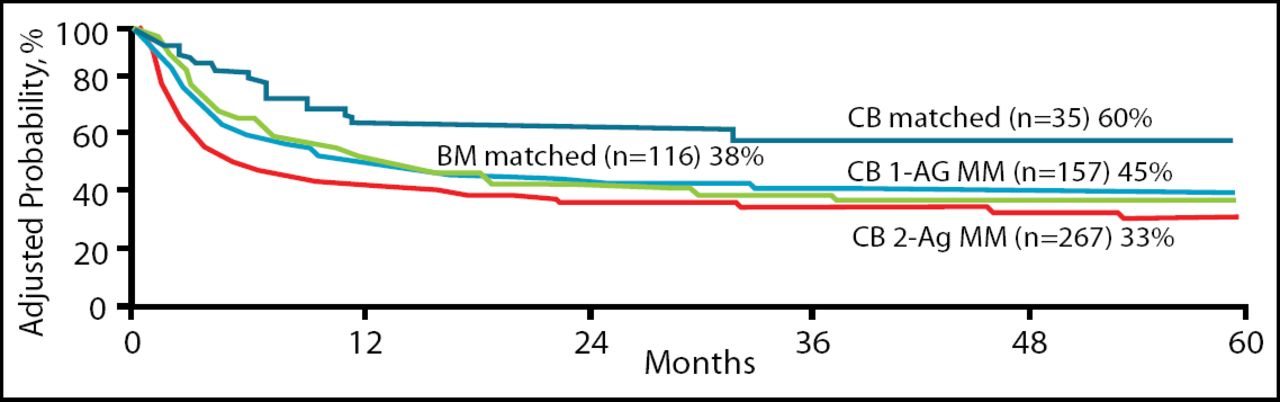
CB Matched and Unmatched Donors vs BM Matched and Unmatched Donors.
Despite the success of UCBT in children, this strategy does not work as well for adults due to low cell doses and mismatches. A new strategy of using a double UCB platform seems to markedly increase the eligibility of adults for UCBT and appears to positively impact survival. Additionally nonmyeloablative therapy clearly extends the eligibility with a low incidence of transplant-related mortality. Finally a new approach that is being developed is to reduce non specific SC losses and optimize homing by direct injection into the pelvis (the BM microenvironment).
In conclusion, allogenic SCT is a viable option for patients without an exact match. Alternatively, recent data has shown that unmatched CB has greater success than either BM or PBSCs that are unmatched. Furthermore, UCBT is the standard of care in children, but the double UCB platform and nonmyeloablative therapy has markedly extended the use of UCBs in adults. It seems that interest in UCB will not wane in the near future as more benefits and applications are being realized.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.