

Summary
Various dietary elements have been linked to the development of colorectal cancer (CRC). In addition, factors like blood lipids could affect how dietary fats contribute to the development of CRC [Kato I et al. Int J Cancer 2010; Endo H et al. Gut 2009]. This article presents the use of data from the Rotterdam Study to determine whether intake of polyunsaturated fatty acids and saturated fatty acids is associated with CRC and whether it is affected by levels of dietary fiber or blood lipids [Kraja B et al. Ann Oncol 2014 (abstr O-0013)].
- Lipid Disorders
- Gastrointestinal Cancers Clinical Trials
- Lipid Disorders
- Gastrointestinal Cancers Clinical Trials
Various dietary elements have been linked to the development of colorectal cancer (CRC). It is not known, however, if or how dietary fat components (eg fatty acids) contribute to this disease. In addition, factors like blood lipids could affect how dietary fats contribute to the development of CRC [Kato I et al. Int J Cancer 2010; Endo H et al. Gut 2009].
Bledar Kraja, MD, PhD, Erasmus Medical Center, Rotterdam, The Netherlands, presented the use of data from the Rotterdam Study to determine whether intake of polyunsaturated fatty acids (PUFAs) and saturated fatty acids (SFAs) is associated with CRC and whether it is affected by levels of dietary fiber or blood lipids [Kraja B et al. Ann Oncol 2014 (abstr O-0013)].
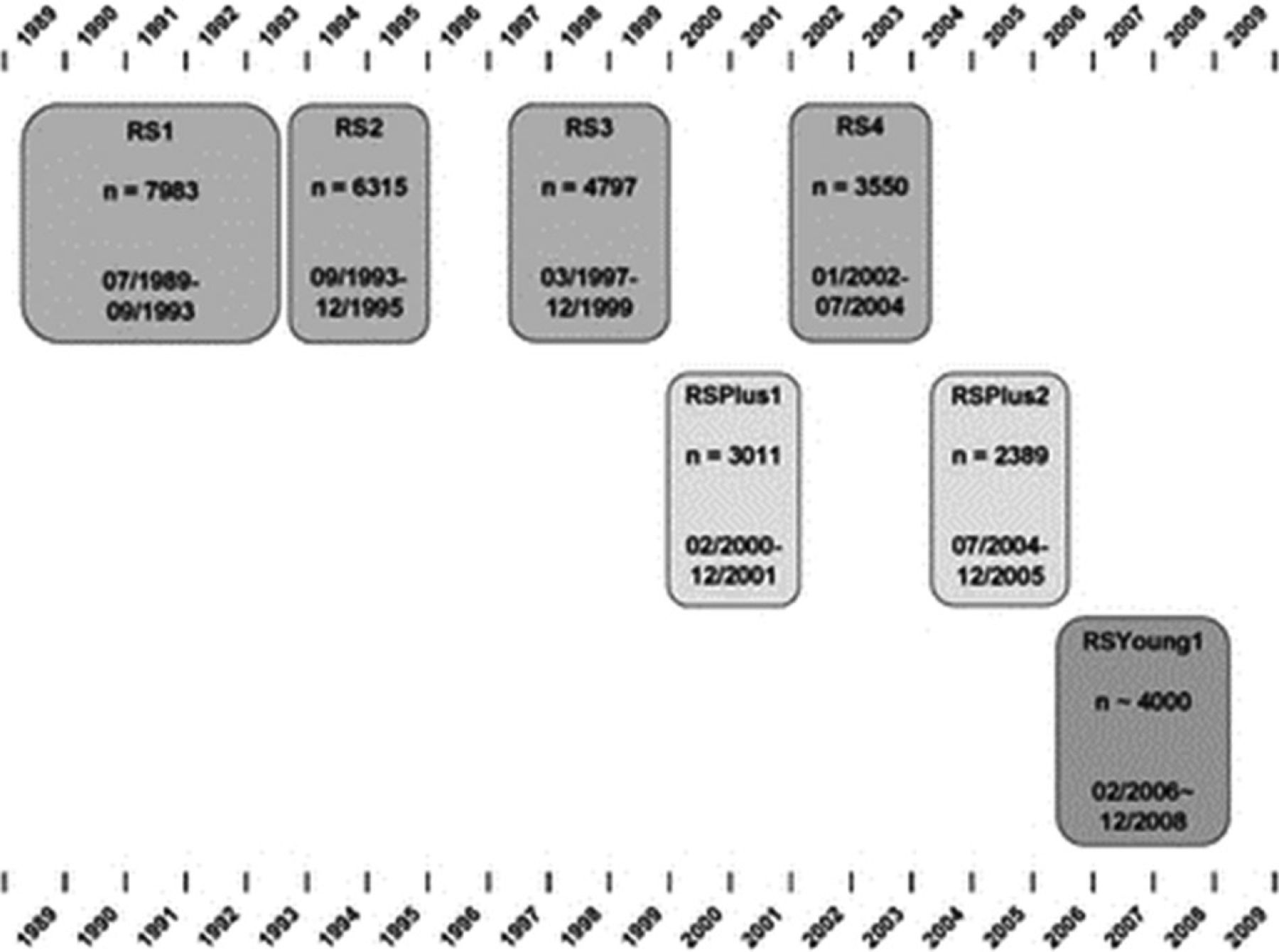
The Rotterdam Study, a single-center, population-based, prospective cohort study that enrolled 7983 adults aged ≥ 55 years in a suburb of Rotterdam, The Netherlands, examined the incidence of, prevalence of, and risk factors for chronic disease in the elderly with the objective of improved prevention and treatment. Researchers obtained baseline measurements from 1990 to 1993, and follow-up measurements every 2 to 3 years for the original cohort. In 2000, 3011 subjects aged ≥ 55 years were added; in 2006, 3932 subjects aged ≥ 45 years were added. All subjects are reexamined every 3 to 4 years. The total Rotterdam Study population includes 14,926 participants [Hofman A et al. Eur J Epidemiol 2013]. The cohorts and examination cycles are shown in Figure 1.

The Rotterdam Study
RS=Rotterdam Study; RS1=baseline examination of original cohort; RS2, RS3, and RS4=reexaminations of the original cohort; RSPlus1=extension of the cohort with individuals in the study district who became age 55 years since the start of the study or those age 55 years or older who migrated into the study district; RSPlus2=reexamination of the extension cohort; RSYoung1=baseline examination of all individuals age 45 years or older living in the study district who had not been examined.
Hofman A et al. The Rotterdam Study: objectives and design update. Eur J Epidemiol. 2007; 22: 819–829. With permission from Springer Publishing Company.
Dr. Kraja's group looked at data from 4902 subjects aged ≥ 55 years from the first cohort of the Rotterdam Study. Diet was determined by a food frequency questionnaire. CRC was classified using the 10th edition of the International Classification of Diseases. Cox regression models were used to calculate multivariable adjusted hazard ratios (HRs).
Incident cases of CRC (n = 218) were identified during a follow-up of 24 years. No evidence of an association between PUFAs intake and CRC was seen. A positive linear relationship was evident, however, between SFAs intake and CRC (HR, 1.02; 95% CI, 1.01 to 1.03). In participants with high dietary-fiber intake (> median), PUFAs intake was associated with an increased risk of CRC (HR, 2.12; 95% CI, 1.04 to 4.29 for the 4th quartile vs the 1st quartile). Among those participants with low fiber intake (< median), SFAs intake was associated with higher CRC risk (HR, 1.52; 95% CI, 1.12 to −2.06 for the 4th quartile vs the 1st quartile). In contrast, a negative linear relationship was observed between SFAs intake and CRC (HR, 0.97; 95% CI, 0.95 to 0.995) among participants with high fiber intake. An increased risk of CRC in participants with low serum cholesterol was associated with a higher PUFAs intake (p interaction = .01 for n-3 PUFA and fiber intake; p interaction = .05 for n-6 PUFAs and serum cholesterol).
Although data from this study suggest that dietary fat intake interacts with dietary fiber and blood lipids to increase the risk of CRC, further investigation is required to determine how other dietary and nondietary factors affect this risk.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.