

Summary
A novel Parachute implant system was found to improve the New York Heart Association (NYHA) class and 6-minute walk distance in patients with heart failure (HF). This article presents data from the Percutaneous Ventricular Restoration in Chronic Heart Failure Due to Ischemic Heart Disease trial.
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Heart Failure
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Heart Failure
- Cardiology
A novel Parachute implant system was found to improve the New York Heart Association (NYHA) class and 6-minute walk distance (6MWD) in patients with heart failure (HF). William T. Abraham, MD, Director of the Division of Cardiovascular Medicine, Ohio State University Wexner Medical Center, Columbus, Ohio, USA, presented data from the Percutaneous Ventricular Restoration in Chronic Heart Failure Due to Ischemic Heart Disease trial.
HF results in at least 1 million hospitalizations per year, with 279,000 deaths and a 5-year mortality rate of about 50% [American Heart Association. Circulation 2014]. After an anterior wall myocardial infarction (AWMI), eccentric wall motion during the AWMI causes left ventricular (LV) remodeling. Over time, the LV enlarges and wall tension rises, which impairs contractility of the myocardium. Therefore, an improvement in LV contraction is needed to resolve symptoms. The purpose of this study was to evaluate the safety and efficacy of the Parachute system in the treatment of HF after a remote MI.
The Parachute system is a collapsible, cuplike implant. Its dual-layer, occlusive membrane is made of polytetrafluoroethylene, which is supported at the edges with polypropylene sutures and a 16-arm frame. A urethane foot at the bottom of the Parachute implant functions as a shock absorber. The implant is delivered and anchored via a 20-cc balloon, which is guided by a catheter (available in 3 sizes). The Parachute implant decreases wall stress in the upper chamber of the heart by decreasing the volume of the LV. It also provides a trampoline effect, replacing scar tissue with a more compliant material that creates an outward force to enhance diastolic filing. Improved diastolic compliance reduces the end-diastolic filling pressure.
The first results from this trial are reported. The cohort comprised 111 consecutive, intent-to-treat patients with NYHA Class III to IV ischemic HF who had received a Parachute implant and were followed for 12 months. These patients were from the USA and Europe, were enrolled on or before December 31, 2012, and were treated for 1 year.
The mean age of the study population was 60.7 years and the mean body mass index was 28.5. Most patients were male (84%). Prior tobacco abuse (74%), hypertension (69%) and diabetes (35%) were common. The use of revascularization with either percutaneous coronary intervention (76%) or coronary artery bypass (17%) or the use of advanced heart failure therapies, such as implantable cardiac defibrillator (38%) or cardiac resynchronization therapy (18%), were also common.
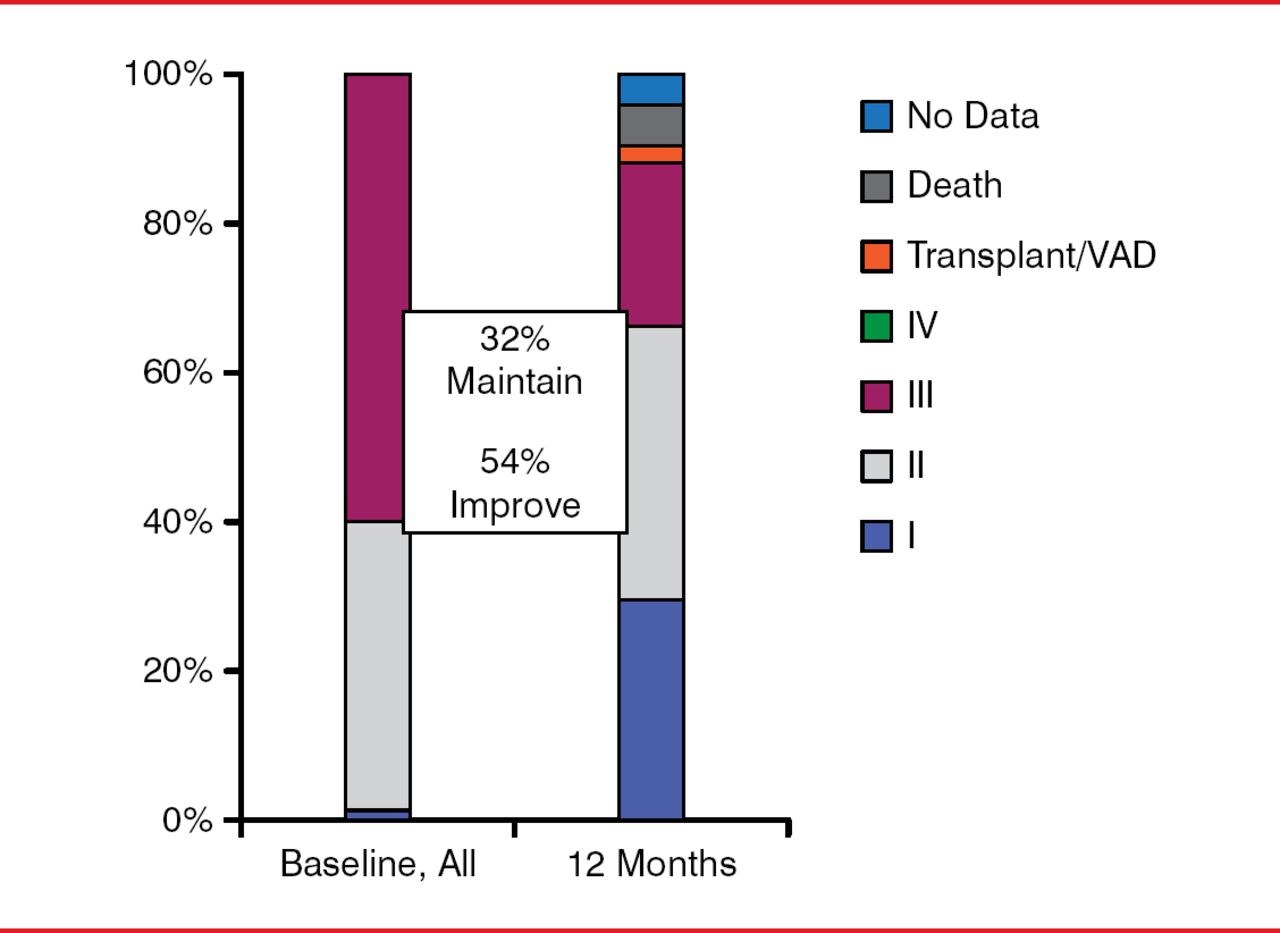
The Parachute implant led to an improvement in NYHA class in 54% patients and maintained the class in 32% patients at the 1-year time point (Figure 1). In addition, patients with the Parachute implant experienced a significant improvement in their 6MWD (p<0.05).

Effect of the Parachute Implant on NYHA Class
NYHA=New York Heart Association.
n=106 and refers to the number of patients discharged with the Parachute device.
*NYHA II at baseline had to be NYHA III or IV in the last 3 months.
Reproduced with permission from WT Abraham, MD.
The 12-month stroke rate was 3%, the all-cause mortality was 6%, and the mortality plus HF hospitalization rate was 22%.
Dr. Abraham concluded that the Parachute implant could benefit some patients with congestive heart failure. The device is currently undergoing further evaluation in the PARACHUTE IV trial, which is now enrolling in the USA [NCT01614652].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.