

Summary
This article discusses the importance of individualizing carbohydrate intake in treating diabetes and shared some of the evidence that was considered when updating the American Diabetes Association (ADA) recommendations [Evert AB et al. Diabetes Care 2014].
- Nutrition Physiology
- Diabetes Mellitus Obesity
- Obesity
- Nutrition Physiology
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
- Obesity
In a symposium on the new “Nutrition Therapy Recommendations for the Management of Adults With Diabetes,” William S. Yancy Jr, MD, VA Medical Center and Duke University School of Medicine, Durham, North Carolina, USA, discussed the importance of individualizing carbohydrate intake in treating diabetes and shared some of the evidence that was considered when updating the American Diabetes Association (ADA) recommendations [Evert AB et al. Diabetes Care 2014].
For many people with diabetes, their biggest challenge is determining what to eat, particularly with respect to carbohydrates. And while the ADA does not recommend any specific eating plan for people with diabetes, it does emphasize that lifestyle and metabolic needs should be considered when choosing one eating pattern over another.
When considering the evidence for patients with diabetes following a low-carbohydrate diet, Dr. Yancy referred to a landmark study involving a strict low-carbohydrate diet in 10 adults with obesity and type 2 diabetes mellitus (T2DM). After following their normal diet for 7 days, participants switched to a low-carbohydrate diet (∼ 21 g/day carbohydrate) for 14 days. The low-carbohydrate diet significantly lowered their levels of plasma glucose (p< .05) and HbA1C (from 7.3% to 6.8%; p< .006) [Boden G et al. Ann Intern Med 2005].
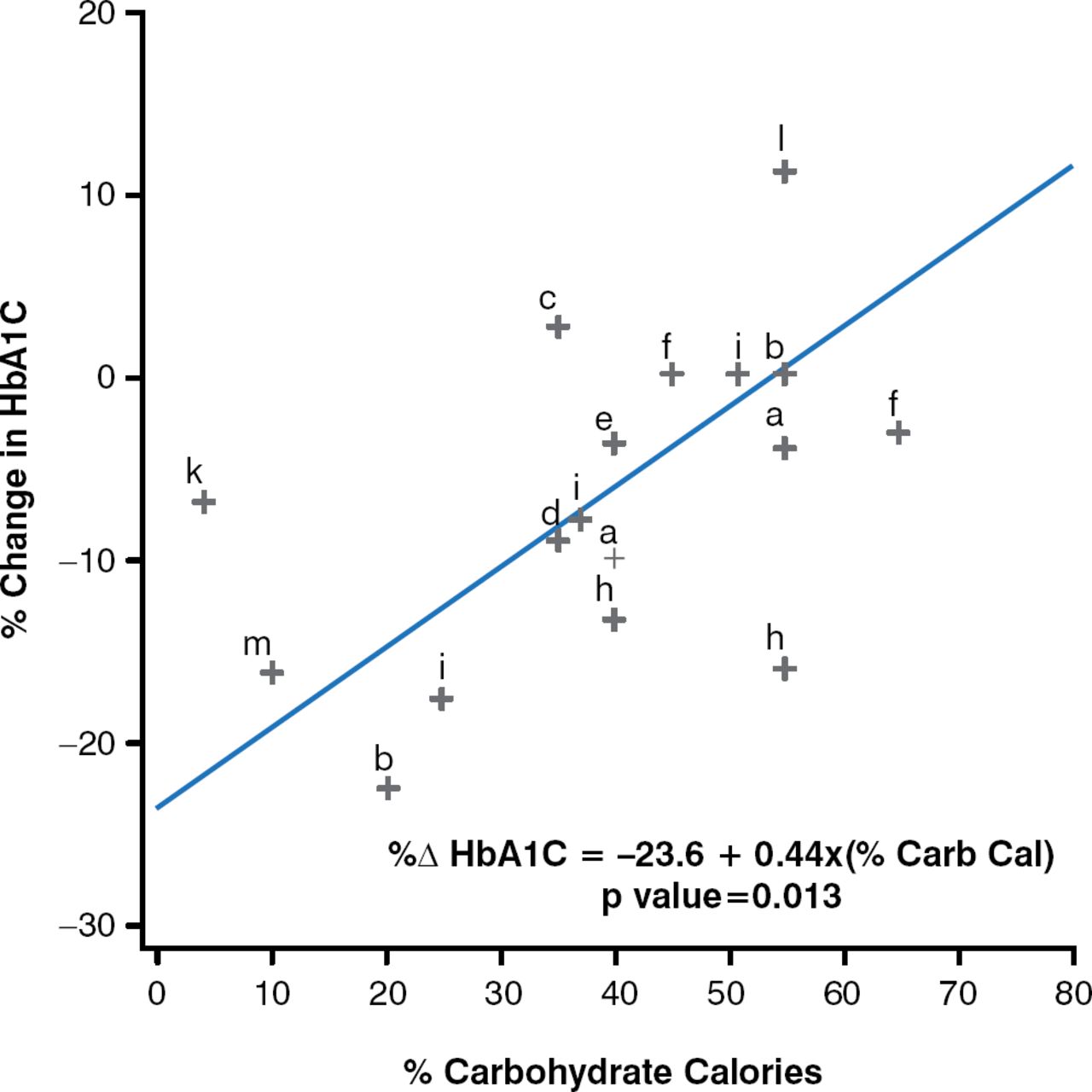
The results of a subsequent meta-analysis of trials evaluating the effects of carbohydrate-restricted diets (< 45% of calories) in patients with T2DM also showed improvements in HbA1C levels as the percentage of calories from carbohydrate was decreased (Figure 1) [Kirk JK et al. J Am Diet Assoc 2008].

Effect of Decreasing Dietary Carbohydrate on HbA1C Levels
Carb cal = carbohydrate calories.
Reproduced from Kirk JK et al. Restricted-carbohydrate diets in patients with type 2 diabetes: a meta-analysis. J Am Diet Assoc. 2008;108:91–100. With permission from Elsevier.
However, Dr. Yancy emphasized that not all studies involving low-carbohydrate diets have shown improvement in glycemic control [Daly ME et al. Diabet Med 2006; Davis NJ et al. Diabetes Care 2009; Iqbal N et al. Obesity 2010]. He also noted that retention levels were low in some studies involving low-carbohydrate diets, and he stressed that this may be one reason why, at this point, such diets have not been endorsed as the superior option for patients with diabetes. Still, the greater glycemic improvement seen in the majority of randomized controlled trials and the potential for reduction in diabetes medications make low-carbohydrate diets a viable treatment option and one worthy of further research.
In contrast, Dr. Yancy remarked that some studies have shown high-carbohydrate diets to be helpful in patients with diabetes. In one study, glycemic and lipid control was improved in participants with T2DM who followed a high-carbohydrate, very-low-fat diet (vegan group), as well as those who followed a moderate-carbohydrate, low-fat diet based on former ADA recommendations. However, the reduction in HbA1C levels was marginally greater for all in the vegan group (p = .09) and significantly greater for those on a stable T2DM medication regimen (p = .01). Also, compared with 26% of the ADA group, 43% of the vegan group reduced the number of diabetes medications during the trial, mainly as necessitated by hypoglycemia [Barnard ND et al. Diabetes Care 2006].
The results of the Look AHEAD (Action for Health in Diabetes) study was also reviewed, which compared the effects of an intensive lifestyle intervention (ILI) with diabetes support and education (DSE) in T2DM [Look AHEAD Research Group. Arch Intern Med 2010]. Data showed that ILI resulted in a greater improvement in HbA1C than did DSE (–0.36% vs −0.09%; p< .001) over a 4-year period.
Consequently, the new recommendations note that the evidence is inconclusive regarding an ideal amount of carbohydrate intake for patients with diabetes, Dr. Yancy stated. He added that while the amount of carbohydrates and available insulin may be the most important factors that influence the glycemic response after eating, higher doses of insulin and several other diabetes medications can lead to unwanted effects, such as weight gain and hypoglycemia. Monitoring carbohydrate intake therefore remains key to glycemic control, and the new recommendations place emphasis on carbohydrate origin. Dr. Yancy concluded that for good health, carbohydrates should come from vegetables, fruits, whole grains, legumes, and dairy products, compared with other sources that contain added fats, sugar, or sodium.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.