

Summary
When discussing diet quality, the ratios of sodium to potassium, calcium, and magnesium may be more important than intake of any one nutrient. One strategy, particularly for heart and bone health, may be a high-quality diet that increases potassium and calcium intake and reduces sodium.
- Nutrition Physiology
- Nutrition
- Nutrition Physiology
When discussing diet quality, the ratios of sodium to potassium, calcium, and magnesium may be more important than intake of any one nutrient. Connie M. Weaver, PhD, Purdue University, West Lafayette, Indiana, USA, believes the best strategy, particularly for heart and bone health may be a high-quality diet that increases potassium and calcium intake and reduces sodium.
Despite long-standing research indicating a direct relationship between sodium intake and cardiovascular (CV) risk, particularly from hypertension, Americans still consume >3400 mg of sodium daily [United States Department of Agriculture (USDA), Agricultural Research Service (ARS). What We Eat in America 2009–2010]. Particularly compelling evidence of the health benefits of a healthy diet combined with a reduction in sodium intake, come from a 2001 study that evaluated the effect of different levels of dietary sodium in conjunction with the Dietary Approaches to Stop Hypertension (DASH) program in persons with and without hypertension [Sacks FM et al. N Engl J Med 2001]. The DASH dietary program encourages the consumption of fruits, vegetables, whole grains, and low-fat dairy foods. It includes meat, fish, poultry, nuts, and beans and is limited in sugar-sweetened foods and beverages, red meat, and added fats. Following the DASH program in conjunction with a reduction in sodium intake substantially lowered blood pressure (BP).
The 2010 Dietary Guidelines for Americans recommend limiting sodium to <2300 mg per day; however, individuals who are aged ≥51 years and those of any age, including children, who are black or have high BP, diabetes, or chronic kidney disease should limit intake to 1500 mg of sodium per day [USDA/Department of Health and Human Services. Dietary Guidelines for Americans, 7th Edition, Washington, DC: US Government Printing Office, December 2010].
In addition to sodium reductions, the 2010 dietary guidelines recommend a daily potassium, calcium, and magnesium intake of 4700 mg (adults), 1000 to 1300 mg (> age 4), and 240 to 420 mg (> age 9), respectively. Animal studies have shown that high potassium intake reduces BP, cerebral vascular lesions, cerebral hemorrhage and mortality, protects against sodium-induced femoral artery intimal thickening, and leads to thinner aortic and mesenteric walls in hypertensive rats. Potassium may also protect against kidney function, interstitial nephritis, and bone resorption.
There is an interactive effect of increased potassium and reduced sodium, where one may modulate the level of the other. Urinary sodium/potassium ratios correct for urine collections and appear to be more informative than either sodium or potassium value alone [Cook NR et al. Arch Intern Med 2009]. A positive relationship (χ2 for trend= −2.69; p=0.007) has been noted between urinary sodium/potassium and stroke mortality in men (aged 40 to 75 years) [He FJ, MacGregor GA. BMJ 2001].
The long-term benefit of increased potassium intake on CV disease (CVD) mortality was shown in a trial in which subjects were switched from regular salt to potassium-enriched salt [Chang HY et al. Am J Clin Nutr 2006]. Fewer CVD-related deaths after 31 months were seen in individuals receiving potassium-enriched salt (HR, 0.59; 95% CI, 0.37 to 0.95; Figure 1).

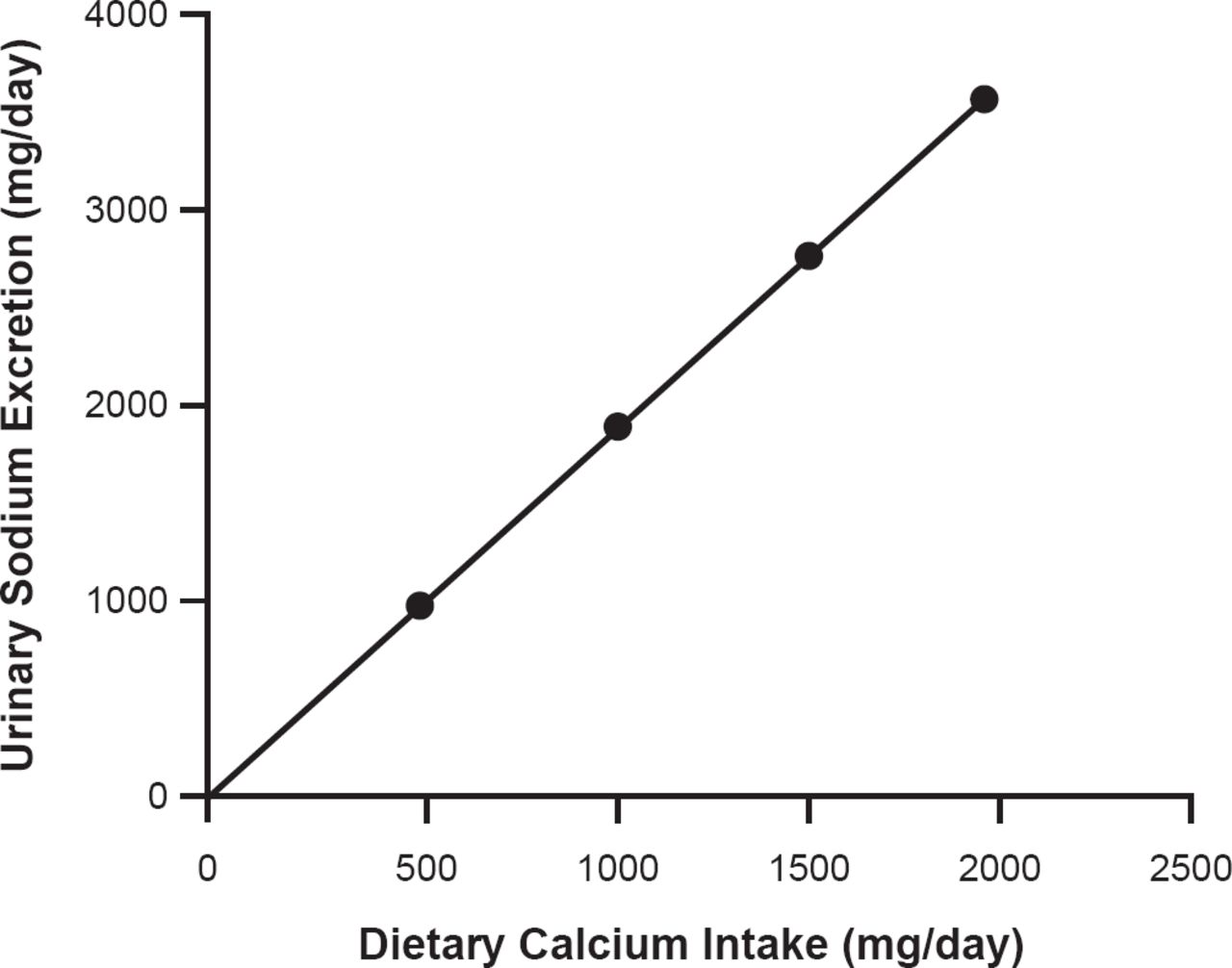
Ratio of Urinary Sodium Excretion to Calcium Intake Needed to Maintain Bone Density
Reproduced with permission from CM Weaver, PhD.
The average intake of potassium in America is 2640 mg/day [USDA, ARS. What We Eat in America 2009–2010], while only 3% of Americans meet recommended adequate in-take for potassium [Fulgoni VL et al. J Nutr 2011]. It is becoming increasing difficult to meet both the sodium and potassium requirements without changes in the current food supply, noted Dr. Weaver.
Dr. Weaver's final topic of discussion was sodium, calcium, and magnesium interactions in adolescents. In a metabolic balance study in black and white girls, sodium retention was higher in black girls compared with white girls [Palacios C et al. J Clin Endocrinol Metab 2004]. As sodium excretion was not greater in blacks, nor did BP or weight increase, the authors speculated that the retained sodium may reside in a nonextracellular compartment, possibly bone. This difference between the two populations may contribute to underlying racial differences in susceptibility to hypertension. In addition, relative to white girls, urinary calcium excretion in black girls is significantly lower with high sodium intake (p<0.05), while calcium retention is higher regardless of sodium intake [Wigertz K et al. Am J Clin Nutr 2005]. These findings may explain racial differences in incidence of hypertension and osteoporosis. Blacks also retain more magnesium regardless of sodium intake [Palacios C et al. Unpublished]. Information regarding the amount of calcium intake and sodium excretion may also be useful for predicting bone loss in postmenopausal women (Figure 1). High-quality diets buffered by increases in potassium and calcium and reductions in sodium may be the best strategy for healthy eating, concluded Dr. Weaver.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.