

Summary
This article discusses the best practices for treating cardiac arrest in the emergency department (ED), emphasizing the need to optimize procedures based on the literature to give patients the best chance for survival. Specific topics include prehospital intubation, intraosseous access, cardiopulmonary resuscitation, and termination of resuscitation, among other topics.
- First Aid
- Transportation Myocardial Infarction
- Critical Care
- First Aid
- Transportation
- Emergency Medicine
- Myocardial Infarction
- Critical Care
Matthew Strehlow, MD, Stanford University, Stanford, California, USA, presented what he considers the best practices for treating cardiac arrest in the emergency department (ED), underscoring the need to optimize procedures based on the literature to give patients the best chance for survival.
Dr Strehlow began with a discussion of prehospital intubation, which remains a controversial topic in part because esophageal intubations are common. There are 2 key steps to check for missed intubations. The first is to monitor end-tidal carbon dioxide (ETCO2). It is also important to ensure that the endotracheal tube (ETT) is not placed too high, which will not be detected with ETCO2 in a patient with spontaneous breathing. Dr Strehlow recommended that every prehospital ETT placement be confirmed either by direct visualization or via video laryngoscopy.
Spontaneous and assisted ventilation has the opposite effects on cardiac output. When a patient is breathing spontaneously, negative pressure draws in air and blood, which increases venous return and cardiac output. In contrast, during assisted ventilation, hyperventilation decreases cardiac output, cerebral perfusion, and coronary perfusion. Dr Strehlow emphasized the importance of not hyperventilating the patient, by having the team leader call out the ventilatory rate and monitor for adherence, with a target of 8 to 10 bag compressions per minute [Neumar RW et al. Circulation. 2010]. He also recommended decreasing the bag size to a 500-mL pediatric Ambu bag in an average-sized adult to further reduce the risk of hyperventilation [Sherren PB et al. Anaesthesia. 2011].
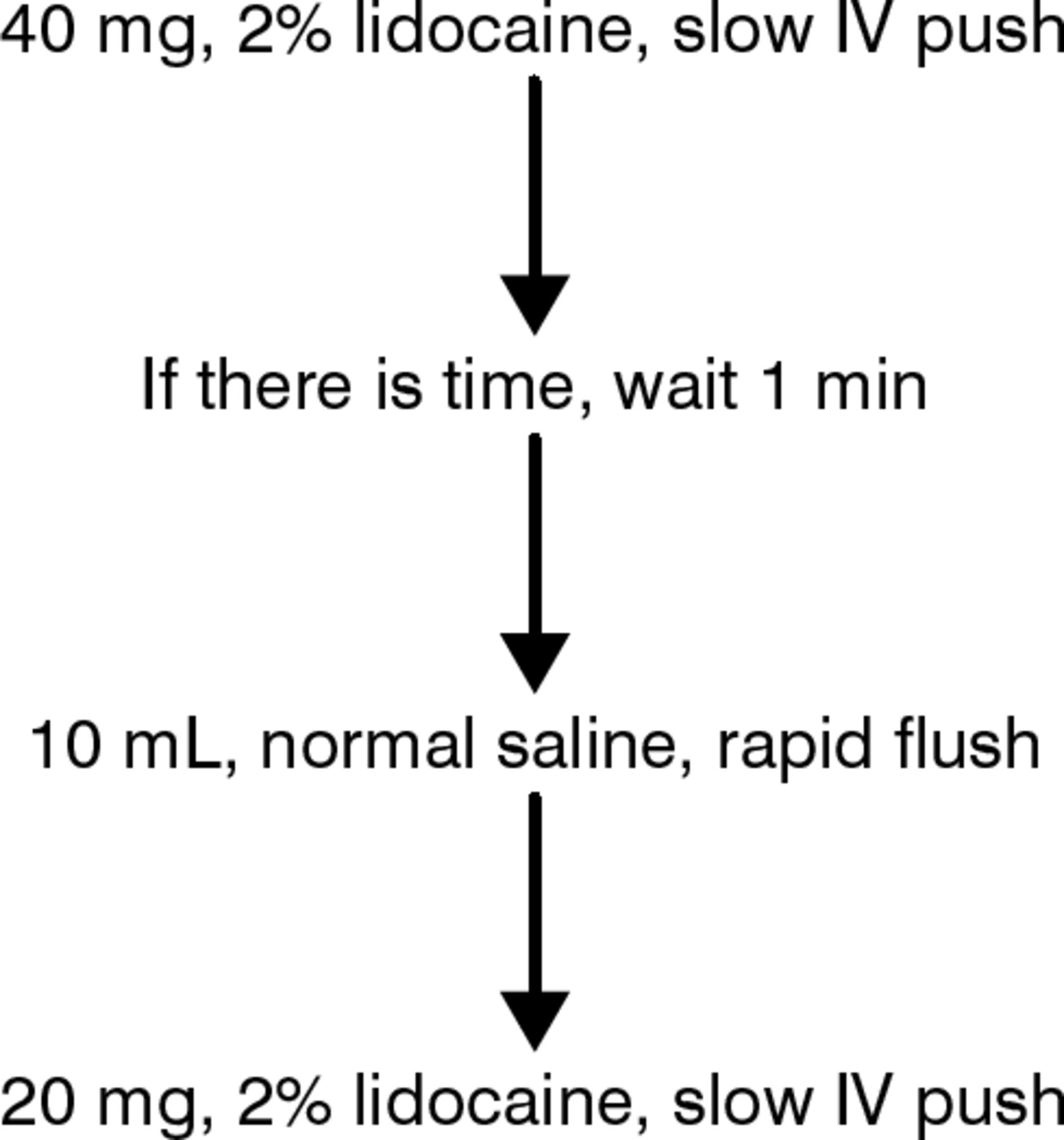
When intravenous (IV) access is difficult, Dr Strehlow endorsed using intraosseous (IO) access in cardiac arrest. Modern IO devices work well, with a first-pass success rate ranging from 85% to 95% [Nagler J et al. N Engl J Med. 2011; Voight J et al. Pediatr Emer Care. 2012]. The proximal tibia is the site typically used in pediatric patients. While this site can also be used in adults, the flow rate will be limited to approximately 1 L/hr. Therefore, for adult patients in cardiac arrest, it is preferable to use the proximal humerus as the IO site. This is a painful procedure for conscious patients, so the proper protocol should be followed to ensure adequate pain control (Figure 1). The rapid flush cleans out the marrow and allows for a faster rate. Any drug may be given via IO, but it is best to switch to IV when possible.

Pain Management Protocol of Intraosseous Device Placement
I V, intravenous.
Source: Miller L et al. Ann Emerg Med. 2010.
Despite guideline recommendations by both the American Heart Association and the International Liaison Committee on Resuscitation regarding the management of cardiac arrest [Circulation. 2005], the IO technique remains underutilized. It is possible that clinicians are concerned about complications; however, the complication rate is similar to that of IV access. The infection rate is < 3%, and the rate of osteomyelitis is < 0.6% [Nagler J et al. N Engl J Med. 2011]. Rates of serious complications, such as infection, compartment syndrome, and bone necrosis, are very rare, and regular checks of the IO site can reduce this risk.
Efforts should also be made to improve cardiopulmonary resuscitation (CPR) techniques. Pauses during CPR should be avoided when possible. If chest compressions stop even for 5 seconds, the coronary perfusion pressure starts to decrease. Compressions should be continued during intubation and defibrillator charging, but Dr Strehlow does not recommend hands-on defibrillation, because the safety is not well established. The 5 essential elements of CPR are presented in Table 1. CPR must be monitored to determine if it is successful. The goal is to achieve diastolic blood pressure > 25 mm Hg. If it falls below 15 mm Hg, the heart will not come back.
Five Essential Elements of Cardiopulmonary Resuscitation
Automated CPR has been promoted as an advance in the management of cardiac arrest. However, the large randomized LINC study [Rubertsson S et al. JAMA. 2014] found no difference in outcome when automated CPR was compared with manual CPR in patients with out-of-hospital cardiac arrest.
Despite research demonstrating that hospitals with longer resuscitation efforts brought more patients back with good neurologic outcomes, according to Dr Strehlow, this does not mean that resuscitation should go on indefinitely [Goldberger ZD et al. Lancet. 2012]. As a measure of perfusion and cardiac output, ETCO2 is a useful tool for determining prognosis. The goal for high-quality CPR is ETCO2 > 20 mm Hg during CPR; with return of spontaneous circulation (ROSC), it will rise to > 30 mm Hg. If ETCO2 is < 10 mm Hg when the patient arrives in the ED, the patient is most likely not going to come back. If after 20 minutes of advanced cardiac life support, the ETCO2 is < 10 mm Hg, the patient is not coming back, and the resuscitation efforts can be stopped [Levine RL et al. N Engl J Med. 1997; Kolar M Critical Care. 2008].
The prehospital basic life support (BLS) rule for termination of resuscitation (TOR) states that if the arrest was not witnessed by emergency medical services (EMS) personnel, if no shock was delivered before transport, and if no ROSC occurred before transport, there is a 99.8% chance that the patient will not survive [Verbeek PR et al. Acad Emerg Med. 2002]. The advanced life support rule for TOR—which is similar to the BLS rule but with the addition of arrest not witnessed by bystander or EMS, and no bystander CPR—predicts 100% mortality [Morrison LJ et al. Resuscitation. 2007].
Dr Strehlow stated that prehospital adoption of these TOR rules should be encouraged and that physicians can be confident in stopping resuscitation efforts if a patient arrives in the ED without having ROSC or meeting either TOR rule.
Dr Strehlow concluded that for a patient in cardiac arrest, the ABCs should be followed: airway, breathing, and circulation. For airway and breathing, confirmation of ETT placement and avoidance of hyperventilation are key. For circulation, IO use should be encouraged and chest compressions optimized.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.