

Summary
This article discusses the results of the Prediction in Intracerebral Hemorrhage [PICH] study. PICH was a prospective observational cohort study which showed that early clinical judgment by attending physicians and nurses more accurately predict 90-day outcome among patients with acute intracerebral hemorrhage compared with two commonly used validated scales.
- Ischemia
- Neurology Clinical Trials
- Ischemia
- Neurology Clinical Trials
- Neurology
David Y. Hwang, MD, Yale School of Medicine, New Haven, Connecticut, USA, presented the results of the Prediction in Intracerebral Hemorrhage study [PICH]. PICH was a prospective observational cohort study which showed that early clinical judgment by attending physicians and nurses more accurately predict 90-day outcome among patients with acute ICH compared with two commonly used validated scales
Determining accurate prognoses for ICH patients is crucial as it drives early decisions regarding life-sustaining therapy, informs patient and family counseling, and influences ICH research including study design and patient enrollment [Holloway RG et al. Neurology 2013]. Although multiple ICH clinical scales have been developed, none have had their accuracy tested against the early judgment of physicians and nurses. The objective of the PICH study was to compare the accuracy of the ICH Score [Hemphill JC et al. Stroke 2001; Neurology 2009] and FUNC score [Rost NS et al. Stroke 2008] with subjective clinical judgment for predicting functional outcome at 3 months among patients with acute ICH. Eligible patients included adults participating in the larger Ethnic/Racial Variations of Intracerebral Hemorrhage (ERICH) study at five centers. Clinician participants comprised of one physician and one nurse caring for each patient. Clinicians were asked to predict the 3-month mRS score for each patient—within 24 hours of each patient admission—and to indicate whether they would recommend comfort care only to the patient's family. ICH and FUNC scores were calculated for each patient upon admission; a blinded 3-month actual mRS was also obtained via ERICH follow-up.
Scores on the ICH scale range from 0 to 6, based on the sum of the scores of 5 components: the Glasgow Coma Scale (GCS) score (counting as 0, 1, or 2 points), ICH volume ≥30 mL, the presence of intraventricular hemorrhage, whether the hemorrhage is of infratentorial origin and, age < or ≥80 years. A score of 6 indicates a high probability for a poor outcome. Among various other outcomes, the ICH score has been validated to predict the probability of achieving functional independence at 90 days. The FUNC score was specifically designed to predict functional independence at 90 days. Scores range from 0 to 11, with a score of 11 indicating the highest probability for favorable outcome. The FUNC score is based on five factors: ICH volume (counting as 0, 2, or 4 points), age (<70, 70 to 79, and ≥80 years; counting as 0, 1, or 2 points), ICH location (lobar, deep, or other; counting as 2, 1, or 0 points), GCS score (counting as 0 or 2 points), and the presence of pre-ICH cognitive impairment.
Of the 405 patients from the ERICH study who were eligible to participate in PICH, 100 were enrolled. Participants were a mean age of 66.8 years; 64% had a GCS score of 13 to 15; the ICH was deep in 53% of patients, lobar in 36%, and infratentorial in 11%. The ICH volume was <30 cc in 70% of patients, between 30 and 60 cc in 16%, and >60 cc in 13%. Among the clinicians, 70% of the physicians were neurologists with 75% of the predictions being made by attending physicians and 25% by trainees. Among the nurses, 71% had a neuroscience specialty.
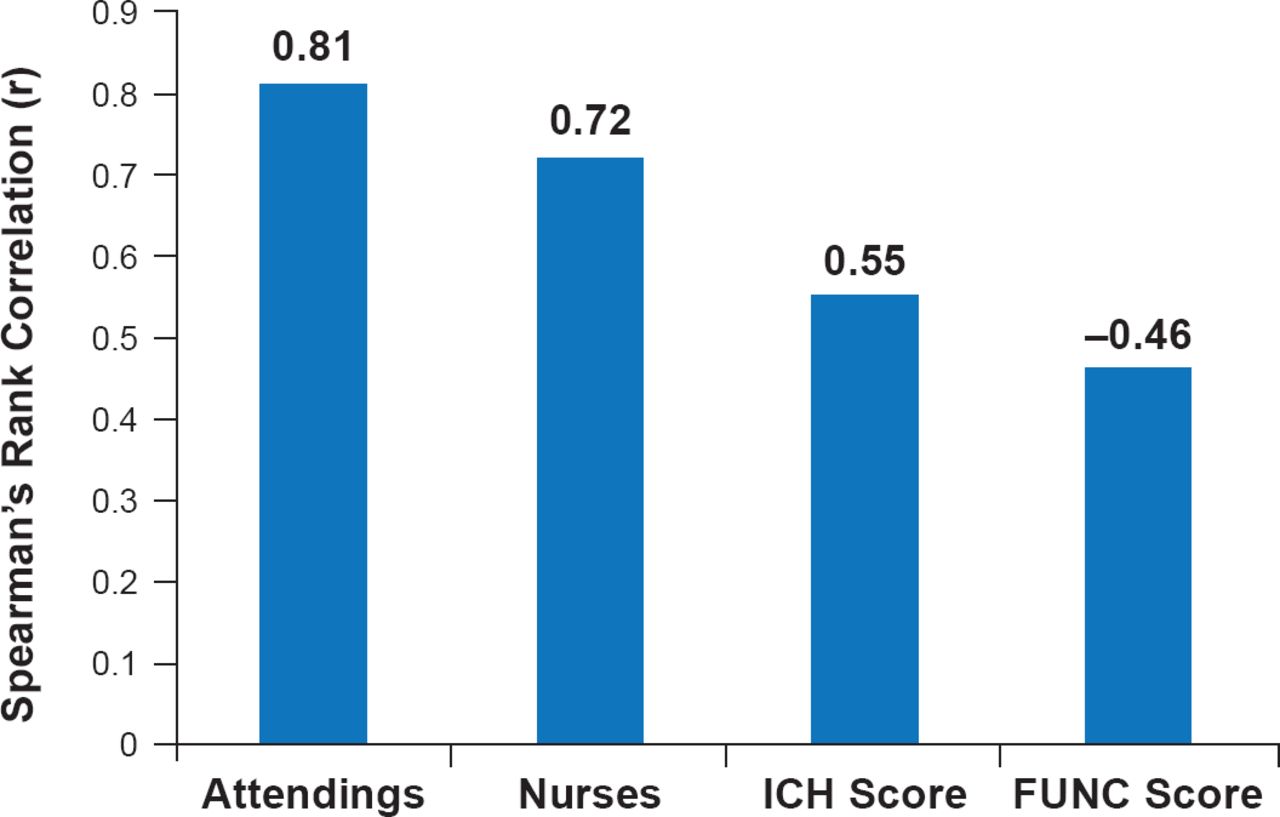
Although all correlations for the clinician predictions and clinical scales with 3-month mRS were significant (p<0.02 for all), the subjective predictions made by both attending physicians and nurses had a higher Spearman's rank correlation with the actual 3-month mRS than either clinical scale (Figure 1).

Correlation of Subjective Predictions and Clinical Scales With Actual 3-Month mRS Score
ICH=intracerebral hemorrhage; all p values <0.05 for comparisons between clinician correlations and ICH/FUNC scores correlations with 3-month mRS. FUNC score correlation is negative since lower score predict poor outcome.
Reproduced with permission from DY Hwang, MD.
When the 18 patients for whom only comfort care was likely recommended were removed from the analysis, the Spearman's rank correlation for the subjective predictions remained higher than those for either clinical score (p<0.05). The results were similar when data for only survivors were analyzed.
The study is limited by several factors: the clinician participants making predictions were not formally trained in the mRS, early predictions were difficult to obtain and led to 218 potential patients being excluded, and, finally, the cohort contained many patients with low GCS and ICH volume.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.